Articles
- Page Path
- HOME > Res Vestib Sci > Volume 18(2); 2019 > Article
-
Case Report
상향안진과 난치성 구토로 발현한 시신경척수염범주질환 -
김현수*, 김재명*, 남태승, 이승한

- Neuromyelitis Optica Spectrum Disorder Presented with Upbeat Nystagmus and Intractable Vomiting
-
Hyunsoo Kim*, Jae-Myung Kim*, Tai-Seung Nam, Seung-Han Lee
-
Research in Vestibular Science 2019;18(2):50-53.
DOI: https://doi.org/10.21790/rvs.2019.18.2.50
Published online: June 15, 2019
Department of Neurology, Chonnam National University Medical School, Chonnam National University Hospital, Gwangju, Korea
- Corresponding Author: Seung-Han Lee Department of Neurology, Chonnam National University Hospital, 42 Jebong-ro, Dong-gu, Gwangju 61469, Korea Tel: +82-62-220-6274 Fax: +82-62-228-3461 E-mail: nrshlee@chonnam.ac.kr
- *These authors contributed equally to this study as co-first authors.
• Received: May 20, 2019 • Revised: June 3, 2019 • Accepted: June 4, 2019
Copyright © 2019 by The Korean Balance Society. All rights reserved.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 6,220 Views
- 89 Download
Abstract
- Neuromyelitis optica spectrum disorder (NMOSD) is an inflammatory demyelinating autoimmune disease of central nervous system characterized by relapsing attacks that target the optic nerves and spinal cord, as well as aquaporin-4 (AQP4) enriched periventricular brain regions. The area postrema (AP), located in the dorsal medulla, is the chemosensitive vomiting center and has high AQP-4 expression. The AP syndrome with unexplained hiccups, nausea, and vomiting is one of the core clinical characteristics in the NMOSD and maybe the first presenting symptom. We experienced a 25-year-old woman presented with intractable vomiting, dizziness and oscillopsia. Upbeat nystagmus detected on the bedside examination led to comprehensive neurological workups including magnetic resonance imaging, and she was diagnosed as the AP syndrome. Ten months later, she experienced a recurrence as a longitudinally extensive transverse myelitis and the diagnosis was finally compatible with NMOSD without AQP4-IgG. NMOSD, especially the AP syndrome, should be considered in any dizzy patient with intractable vomiting, and detailed neuro-otologic and neuro-ophthalmologic examinations are warranted for the correct diagnosis.
서 론
증 례
고 찰
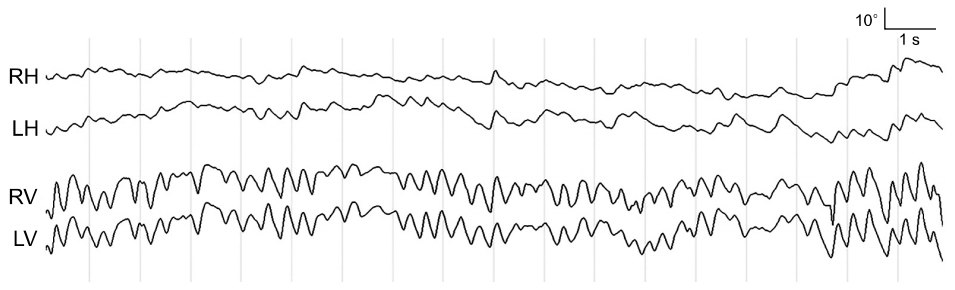
Fig. 1.Video-oculography. Video-oculography without fixation condition shows spontaneous upbeat nystagmus on both eyes (maximal slow phase velocity=56 °/sec). The upbeat nystagmus is accompanied by subtle right beating-components in both eyes. RH, horizontal position of right eye; LH, horizontal position of left eye; RV, vertical position of right eye; LV, vertical position of left eye.
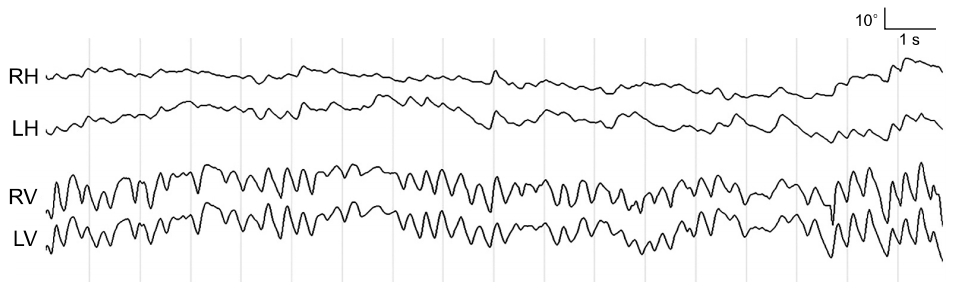
Fig. 2.Brain magnetic resonance imaging. T2-weighted (A, B) and fluid attenuated inversion recovery (C, D) images demonstrate bilateral symmetric high signal intensities (arrows) in the dorsal medulla, suggesting area postrema syndrome.
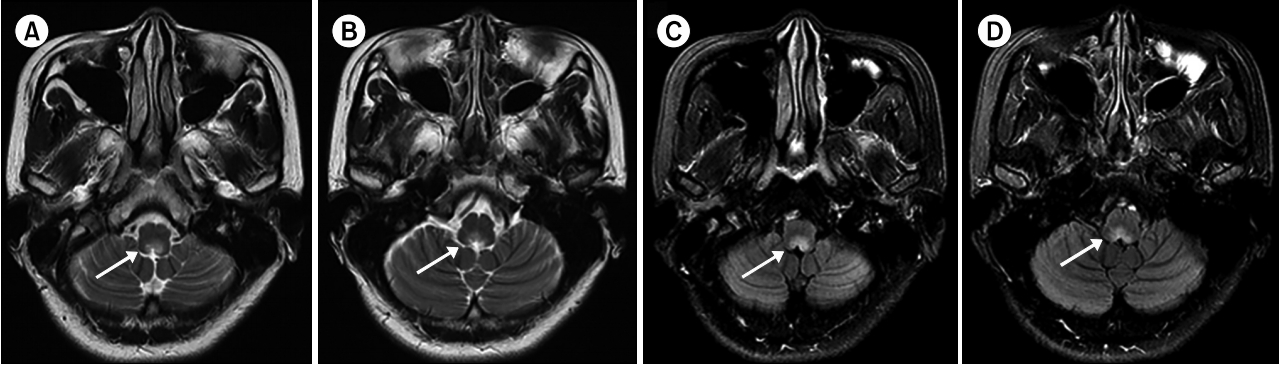
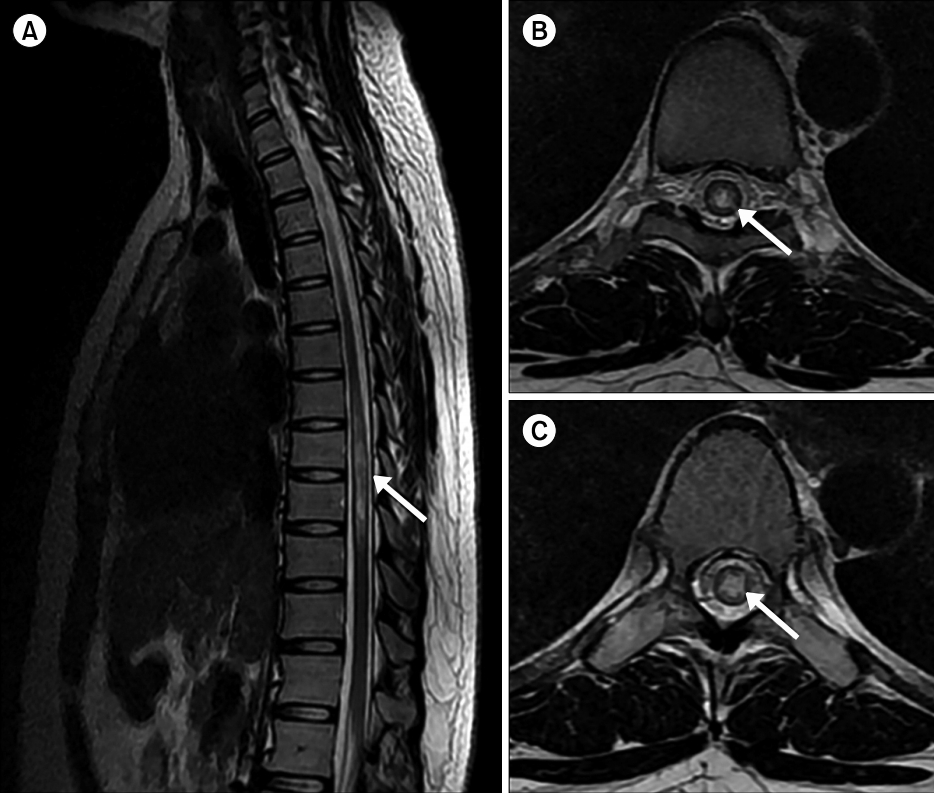
Fig. 3.Spine magnetic resonance imaging. (A) Sagittal T2-weighted image shows high signal intensities in the thoracic spinal cord from T7 to T11 vertebral segments which are compatible with longitudinally extensive transverse myelopathy (arrow). (B, C) Axial T2-weighted images reveal predominant involvement of the central gray matter of the thoracic spinal cord, which is a supportive finding of neuromyelitis optica spectrum disorder (arrows).
- 1. Wingerchuk DM, Hogancamp WF, O'Brien PC, Weinshenker BG. The clinical course of neuromyelitis optica (Devic's syndrome). Neurology 1999;53:1107–14.ArticlePubMed
- 2. Wingerchuk DM, Banwell B, Bennett JL, Cabre P, Carroll W, Chitnis T, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 2015;85:177–89.ArticlePubMedPMC
- 3. Frigeri A, Gropper MA, Turck CW, Verkman AS. Immunolocalization of the mercurial-insensitive water channel and glycerol intrinsic protein in epithelial cell plasma membranes. Proc Natl Acad Sci U S A 1995;92:4328–31.ArticlePubMedPMC
- 4. Pittock SJ, Weinshenker BG, Lucchinetti CF, Wingerchuk DM, Corboy JR, Lennon VA. Neuromyelitis optica brain lesions localized at sites of high aquaporin 4 expression. Arch Neurol 2006;63:964–8.ArticlePubMed
- 5. Shosha E, Dubey D, Palace J, Nakashima I, Jacob A, Fujihara K, et al. Area postrema syndrome: Frequency, criteria, and severity in AQP4-IgG-positive NMOSD. Neurology 2018;91:e1642–51.ArticlePubMedPMC
- 6. Misu T, Fujihara K, Nakashima I, Sato S, Itoyama Y. Intractable hiccup and nausea with periaqueductal lesions in neuromyelitis optica. Neurology 2005;65:1479–82.ArticlePubMed
- 7. Apiwattanakul M, Popescu BF, Matiello M, Weinshenker BG, Lucchinetti CF, Lennon VA, et al. Intractable vomiting as the initial presentation of neuromyelitis optica. Ann Neurol 2010;68:757–61.ArticlePubMed
- 8. Pierrot-Deseilligny C, Milea D. Vertical nystagmus: clinical facts and hypotheses. Brain 2005;128(Pt 6):1237–46.ArticlePubMedPDF
- 9. Kim JS, Yoon B, Choi KD, Oh SY, Park SH, Kim BK. Upbeat nystagmus: clinicoanatomical correlations in 15 patients. J Clin Neurol 2006;2:58–65.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader ePub Link
ePub Link Cite
Cite