Abstract
- Developmental venous anomalies (DVAs), previously known as central nervous system venous angioma, are the commonly encountered benign vascular malformations. Unlike cerebellar DVAs, isolated brainstem DVAs is a rare condition, and there have been limited case reports of symptomatic and uncomplicated DVAs of the brainstem described in the literature. We present the exceptional case of spontaneous vertigo accompanied by moderate temporal headache associated with pontine DVAs. To the best of our knowledge, this is one of the first documented cases of DVAs as a possible cause of spontaneous recurrent vertigo.
-
Keywords: Central nervous system venous angioma; Vertigo; Brainstem
-
중심단어: 중추신경계 정맥혈관종, 현훈, 뇌간
INTRODUCTION
Developmental venous anomalies (DVAs), previously known as central nervous system venous angioma, are the commonly encountered benign vascular malformations which account for over 60% of all cerebral vascular malformations— coexistent of a malformation of medullary veins and normal brain parenchyma [1]. Although DVAs are generally considered as benign lesions that may uncommonly present symptomatically, the most common clinical presentation is headache, focal neurologic deficits, and seizures [1,2]. We present the case of pontine DVAs in a 15-year-old girl with a 5-year history of spontaneous vertigo accompanied by moderate temporal headache; the clinical presentation, the audio-vestibular function test, and the radiologic findings are discussed.
CASE REPORT
A 15-year-old girl presented with a 5-year history of recurrent vertigo that occurred more than three times a day and lasted about 15 minutes, accompanied by moderate headache of both temporal areas. She had no current or previous history of migraine and the clinical symptoms did not fulfill the criteria of vestibular migraine according to the Barany Society and the International Headache Society [3]. The physical examination and otoscopy yielded normal findings. During the evaluation, pure tone audiometry, vestibular function test including video nystagmography, caloric test, video head impulse test (vHIT), and magnetic resonance imaging (MRI) with angiography were performed. Pure tone audiometry showed normal hearing status. Video nystagmography showed neither spontaneous nystagmus nor gaze-evoked nystagmus (GEN). In the saccadic eye movement test, hypometria was predominantly observed on the right eyeball in bilateral horizontal measurements (Fig. 1A). In addition, caloric test showed mild right-sided weakness with canal paresis ratio of 22.09%, but vHIT showed normal findings at three semicircular canals (Fig. 1B, C). The MRI with angiography revealed DVAs in the right ventral pons and medulla in proximity to the vestibular nuclei complex. There was no evidence of a cavernous angioma, hemorrhage, acute parenchymal injury, or edematous changes. Axial T1-weighted turbo spin-echo gadolinium MRI showed a vascular-like enhancement presenting radicular divisions in the pons extending to medulla oblongata having a caput medusae appearance (Fig. 2). The DVAs were considered to be the cause of clinical symptoms because all other causes were excluded at physical examination, the audio-vestibular function test, and the radiologic examination. Empirical treatment to alleviate symptoms with beta- adrenergic blocking agents to lower the blood pressure in enlarged veins in DVAs was followed. The patient reported partial resolution of symptoms with medication in less than 50% of vertigo attacks. Conservative management for symptom control with regular follow-up appointments was recommended.
Fig. 1.(A) Hypometric movement was observed in saccadic test. Caloric test (B) showed mild right-sided weakness with canal paralysis ratio of 22.09% and video head impulse test (C) showed normal findings at three semicircular canals. PR, PR score (coefficient of variance); NA, non available.
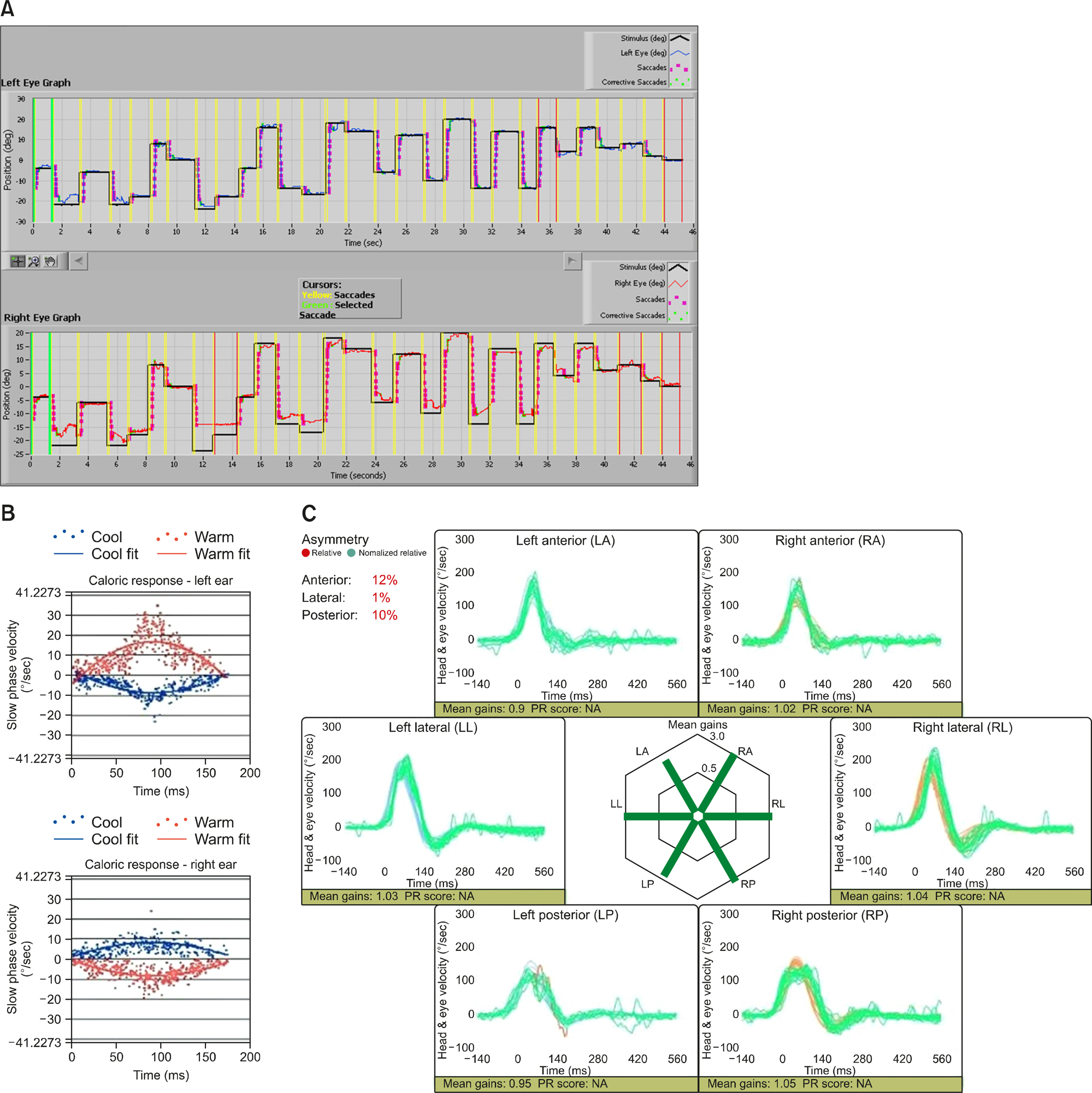
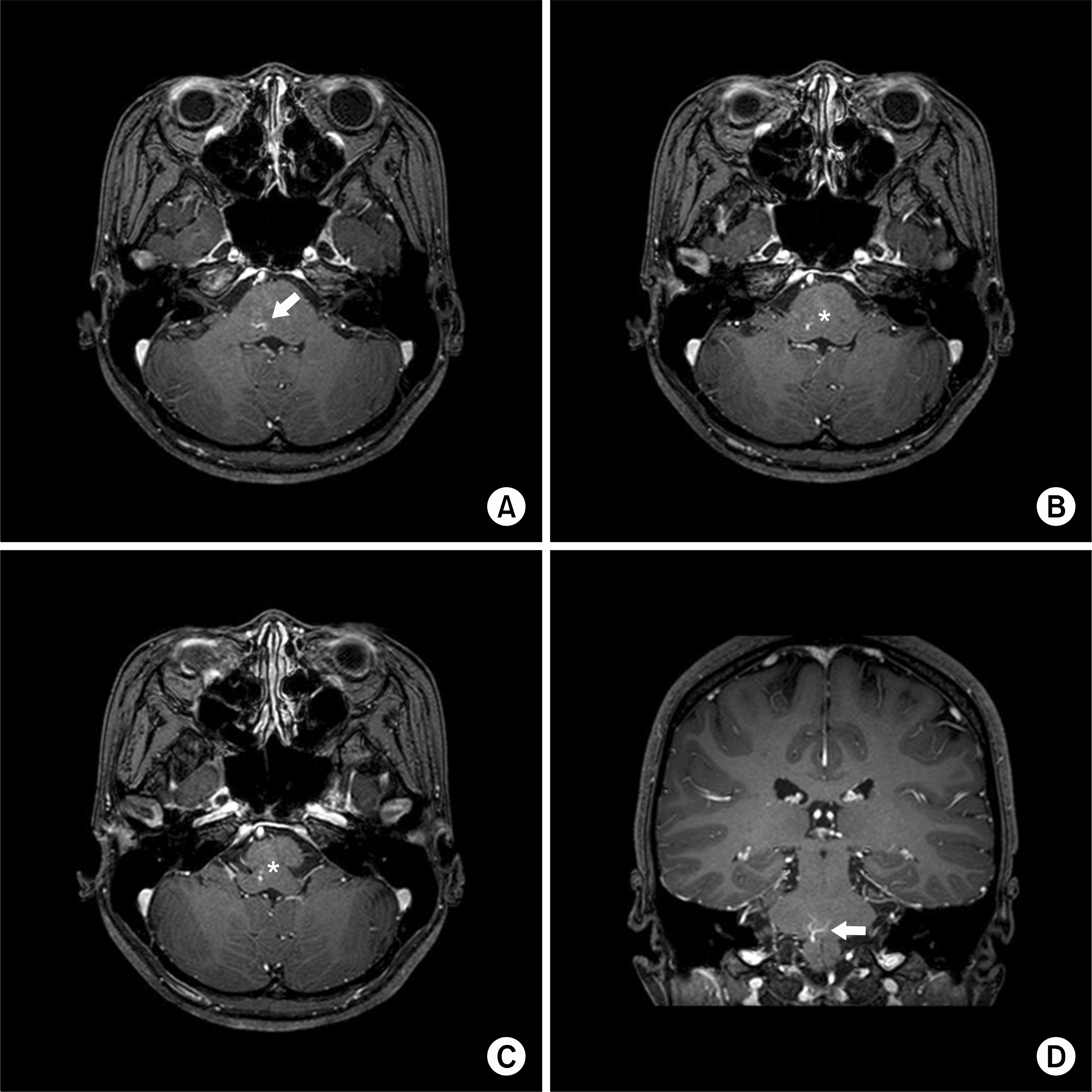
Fig. 2.Four selected images from axial and coronal T1-weighted turbo spin-echo gadolinium magnetic resonance imaging sequence acquisition show a vascular-like contrast enhancement, or “caput medusae” (A and D; arrows), consistent with a developmental venous anomaly, from the right pons to medullar oblongata (B and C) with a drainage vein (asterisks).

This study was approved by the Institutional Review Board of Yonsei University College of Medicine (No. 3-2020-0331). The written informed consent and permission to publish the clinical images were obtained from the patient.
DISCUSSION
DVAs are congenital venous malformation mostly without clinical presentation. DVAs represent remaining fetal venous drainage failed to develop a normal adult venous system [1]. Uncomplicated DVAs without hemorrhage remain asymptom-atic in most cases and are frequently diagnosed incidentally by radiologic studies of brain. Neurological symptoms such as vertigo, ataxia, and headache are rarely accompanied [2]. The location of DVAs is various, among which the cerebellum and the brainstem account for about one out of three [4]. Diagnosis is made on demonstrating a caput medusae in imaging, an engorged collecting vein with radiating small venules. Without ischemic or hemorrhagic complications, the clinical significance of DVAs is controversial. Management of uncomplicated DVAs remains uncertain. However, surgical intervention of uncomplicated DVAs is generally contraindicated, because risk of hemorrhagic complication is higher (0.22% per year) than risk of spontaneous hemorrhage [5].
Network of abnormal veins in DVAs compensates insufficient draining veins in brain parenchyma, however which can cause venous congestion and hypertension resulting in parenchymal infarction [6]. It is suggested that venous hypertension was the common factor to cause abnormalities of cerebral parenchyma in DVAs [7]. Venous congestion followed by interstitial edema could be responsible for dysfunction around the location of DVAs [8]. Hence DVAs may cause various clinical presentations correlated to the location of malformation. Permanent tinnitus can be triggered by DVAs crossing the origin of the acousticofacial bundle exerting pressure on the nerve and gait abnormality with ipsilateral temporal headache can be caused by DVAs in the cerebellopontine angle adjacent to the vestibulocochlear nerve [6,9].
Our patient presented with spontaneous recurrent vertigo accompanied by moderate headache of both temporal areas. The vestibular nuclei complex is mainly located in the pons extending rostrally to the floor of the cerebellum and caudally into the medulla [10]. The DVAs of the patient was located adjacent to the vestibular nuclei complex. Venous congestion and interstitial edema around the lesion can cause imbalance of vestibular firing rate of the vestibular nuclei complex, which can result in vertigo attack. Venous hypertension can be transient and repetitive provoking recurrent attacks. The location of DVAs was also adjacent to paramedian pontine reticular formation along with the vestibular nuclei complex which organizes the neuronal information in saccade pathway. Hypometric saccade movement in both directions seems compatible with a dysfunction of the affected area. Although there is no pathognomonic nystagmus associated with DVAs, nystagmus of many forms can be shown including single-sided gaze nystagmus, GEN, and upbeating nystagmus at particular gaze [8].
In conclusion, this rare case report illustrates that uncomplicated symptomatic pontine DVAs. We speculate that the symptoms were caused by venous hypertension of the DVAs adjacent to vestibular nuclei. Evident finding suggesting brainstem dysfunction during vertigo attacks was limited because diagnostic workups were not performed during the attacks. However, differential diagnosis with thorough review of symptoms, physical examination, various audio-vestibular function tests, and imaging evaluation made it conceivable that the DVAs caused the symptoms. Although brainstem DVAs are rare, they need to be considered in the differential diagnosis of recurrent spontaneous vertigo. MRI with angiography is the modality of choice in the differential diagnosis of vascular malformation associated with a higher risk of hemorrhage and also useful for follow-up.
ARTICLE INFORMATION
-
No potential conflict of interest relevant to this article was reported.
REFERENCES
- 1. Pereira VM, Geibprasert S, Krings T, Aurboonyawat T, Ozanne A, Toulgoat F, et al. Pathomechanisms of symptomatic developmental venous anomalies. Stroke 2008;39:3201–15.ArticlePubMed
- 2. Naff NJ, Wemmer J, Hoenig-Rigamonti K, Rigamonti DR. A longitudinal study of patients with venous malformations: documentation of a negligible hemorrhage risk and benign natural history. Neurology 1998;50:1709–14.ArticlePubMed
- 3. Lempert T, Olesen J, Furman J, Waterston J, Seemungal B, Carey J, et al. Vestibular migraine: diagnostic criteria. J Vestib Res 2012;22:167–72.ArticlePubMed
- 4. Töpper R, Jürgens E, Reul J, Thron A. Clinical significance of intracranial developmental venous anomalies. J Neurol Neurosurg Psychiatry 1999;67:234–8.ArticlePubMedPMC
- 5. Ferreira D, Mendes V, Vide A, Costa JD. Developmental venous anomaly of the internal auditory canal in a child with unilateral sensorineural hearing loss–a rare association. Pediatr Radiol 2012;42:1021–3.ArticlePubMed
- 6. Malinvaud D, Lecanu JB, Halimi P, Avan P, Bonfils P. Tinnitus and cerebellar developmental venous anomaly. Arch Otolaryngol Head Neck Surg 2006;132:550–3.ArticlePubMed
- 7. San Millán Ruíz D, Delavelle J, Yilmaz H, Gailloud P, Piovan E, Bertramello A, et al. Parenchymal abnormalities associated with developmental venous anomalies. Neuroradiology 2007;49:987–95.ArticlePubMed
- 8. Fenzi F, Rizzuto N. Ataxia and migraine-like headache in a girl with a cerebellar developmental venous anomaly. J Neurol Sci 2008;273:127–9.ArticlePubMed
- 9. Augenstein JA, Chapman T, McNeil MJ, Lo MD. “It's not a tumor”: a rare case of symptomatic cerebellar developmental venous anomaly. Pediatr Emerg Care 2019;35:e40–1.ArticlePubMed
- 10. Barmack NH. Central vestibular system: vestibular nuclei and posterior cerebellum. Brain Res Bull 2003;60:511–41.ArticlePubMed
Citations
Citations to this article as recorded by




 PubReader
PubReader ePub Link
ePub Link Cite
Cite