Abstract
- Vertebral artery dissection (VAD) during a golf swing is extremely rare. Golf- related VAD has been reported to occur more commonly at extracranial segments on the right side. In the present study, we report a 57-year-old, right-handed, female amateur golfer with golf-related VAD which developed at the intracranial segment (V4) of the left vertebral artery. The patient complained of sudden vertigo with nausea and vomiting, and aggravation of the left tinnitus. Video oculo-graphy showed very weakly left- and upbeating spontaneous nystagmus. The intensity of nystagmus was increased by positioning such as bowing, lying down or right head-rolling. The patient was treated with oral aspirin, and complete recanalization of the left vertebral artery was observed in a follow-up imaging study.
-
Keywords: Vertebral artery; Dissection; Golf; Vertigo; Headache
INTRODUCTION
Arterial dissection is a result of blood entering the tunica media through a tear in the tunica intima. Although vertebral artery dissection (VAD) does not occur frequently, it is known as a leading cause of stroke in young and otherwise healthy individuals. VAD during a golf swing is an extremely rare condition, and only a few cases have been reported [1–5]. Quick rotation of the neck during a golf swing is considered as a cause of stretch and twist of the vertebral artery [1,2]. In the present study, we describe a new case of VAD in an amateur golfer and discuss the mechanism of the nystagmus observed in this patient.
CASE REPORT
A previously healthy, 57-year-old, right-handed, female amateur golfer swung a driver with nearly maximal force while practicing golf at the driving range. Severe pain suddenly developed in her left neck, which was spreading to the left occipital area. She visited local hospital and was prescribed some headache pills. The symptoms gradually improved, and she continued practicing golf swing. Seven days later, she felt severe vertigo with nausea and vomiting, and aggravation of tinnitus developed on the left side during golf swing.
The patient reported that vertigo was aggravated by changing the head position, although she could not specify which head position the vertigo was getting worse. Head rotation to either side in a sitting position, which was performed to rule out rotational vertebral artery occlusion (RVAO), did not elicit worsening of vertigo or tinnitus. Physical examination revealed no other additional neurological deficits.
Video oculography showed very weakly left (maximal slow- phase velocity, mSPV; 2°/sec) and upbeating (mSPV, 1°/sec) spontaneous nystagmus (Supplementary Video 1). The intensity of nystagmus was increased by positioning such as bowing (mSPV, 5°/sec to the rightward and 1°/sec to the downward), lying down (mSPV, 3°/sec to the rightward and 4°/sec to the downward) or right head-rolling (mSPV, 4°/sec to the rightward and 4°/sec to the downward) (Supplementary Video 1). Aug-mentation of spontaneous nystagmus was observed after hori-zontal head-shaking (mSPV, 6°/sec to the rightward), and vertical head-shaking (mSPV, 5°/sec to the downward) (Sup-plementary Video 2).
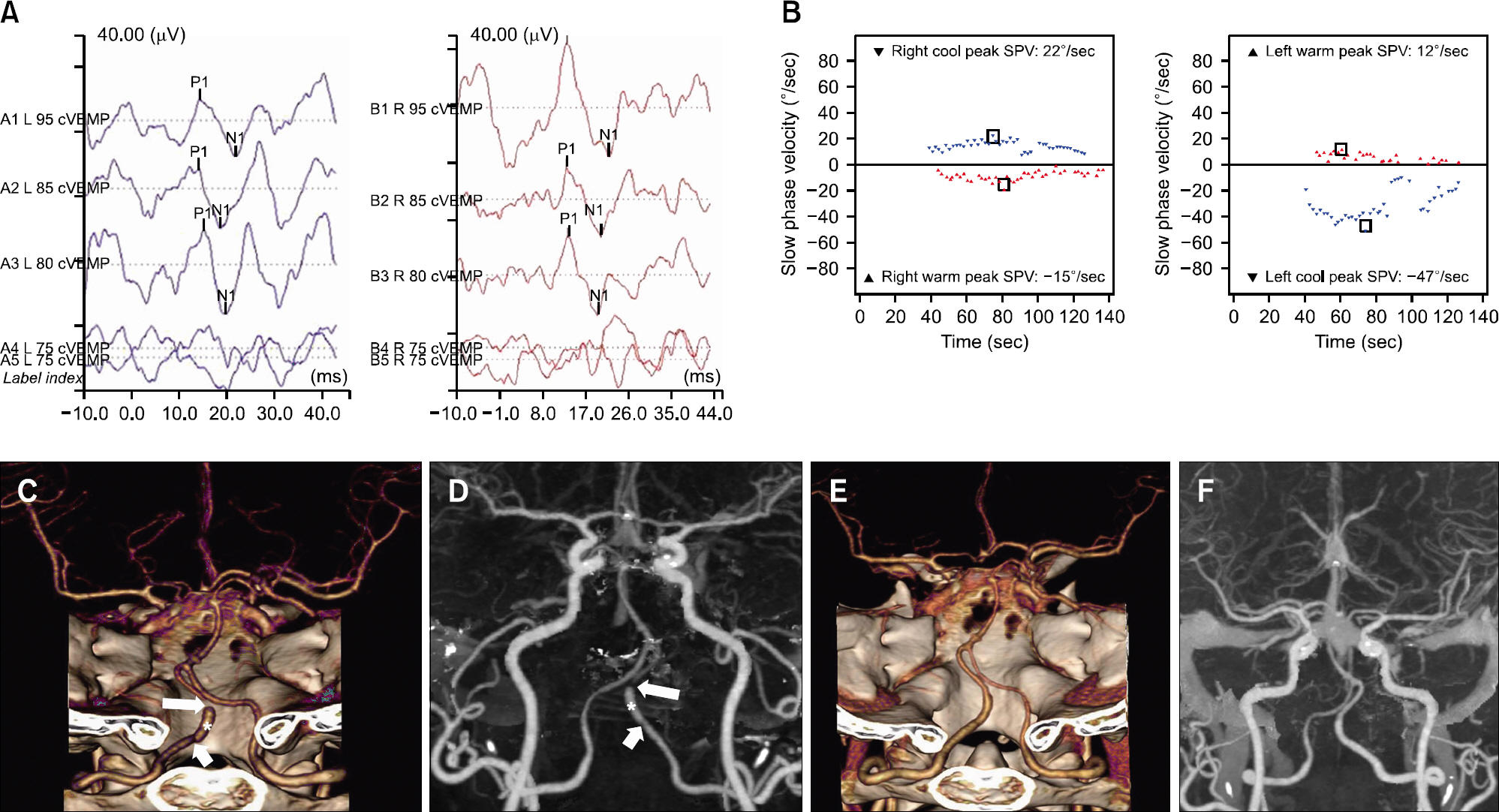
The average threshold of pure tone audiometry (0.5+1+2+3 kHz/4) was 18.8 dB on the right and 23.8 dB on the left side. The cervical vestibular-evoked myogenic potential test showed decreased amplitude on the left side, and the interaural amp-litude difference ratio was 39.8% (Fig. 1A). A bithermal caloric test revealed no canal paresis on either side (Fig. 1B). Brain magnetic resonance imaging including diffusion-weighted im-aging showed no acute infarction or other abnormalities. Three- dimensional computed tomographic angiography (3D-CTA) re-vealed focal aneurysmal dilatation (asterisks in Fig. 1C, D) of the V4 segment of the left vertebral artery. Focal indentation at the proximal end (short arrows in Fig. 1C, D) and severe stenosis (long arrows in Fig. 1C, D) at the distal end of aneurysmal dilatation of the left vertebral artery were identified due to dissection.
Fig. 1.(A) In cervical vestibular-evoked myogenic potential test, the peak-to-peak amplitude at 95 dB nHL was 80.12 μ V on the right side and 34.49 μV on the left side. (B) A bithermal caloric test revealed no canal paresis on either side. Posterior view of volume rendering (VR, C) and anteroposterior view of maximal intensity projection (MIP, D) images of cerebral computed tomographic angiography (CTA) showed focal aneurysmal dilation (asterisks) of the V4 segment of the left vertebral artery. Focal indentation at the proximal end (short arrows) and severe stenosis (long arrows) at the distal end of aneurysmal dilation of the vertebral artery were identified due to dissection. On follow-up VR (E) and MIP (F) images of cerebral CTA in 2 months, previously noted aneurysmal dilation, distal stenosis, and proximal indentation in left vertebral artery disappeared. These images demonstrate healed stage of dissection involving V4 segment of the left vertebral artery. cVEMP, cervical vestibular-evoked; SPV, slow phase velocity; L, left; R, right.
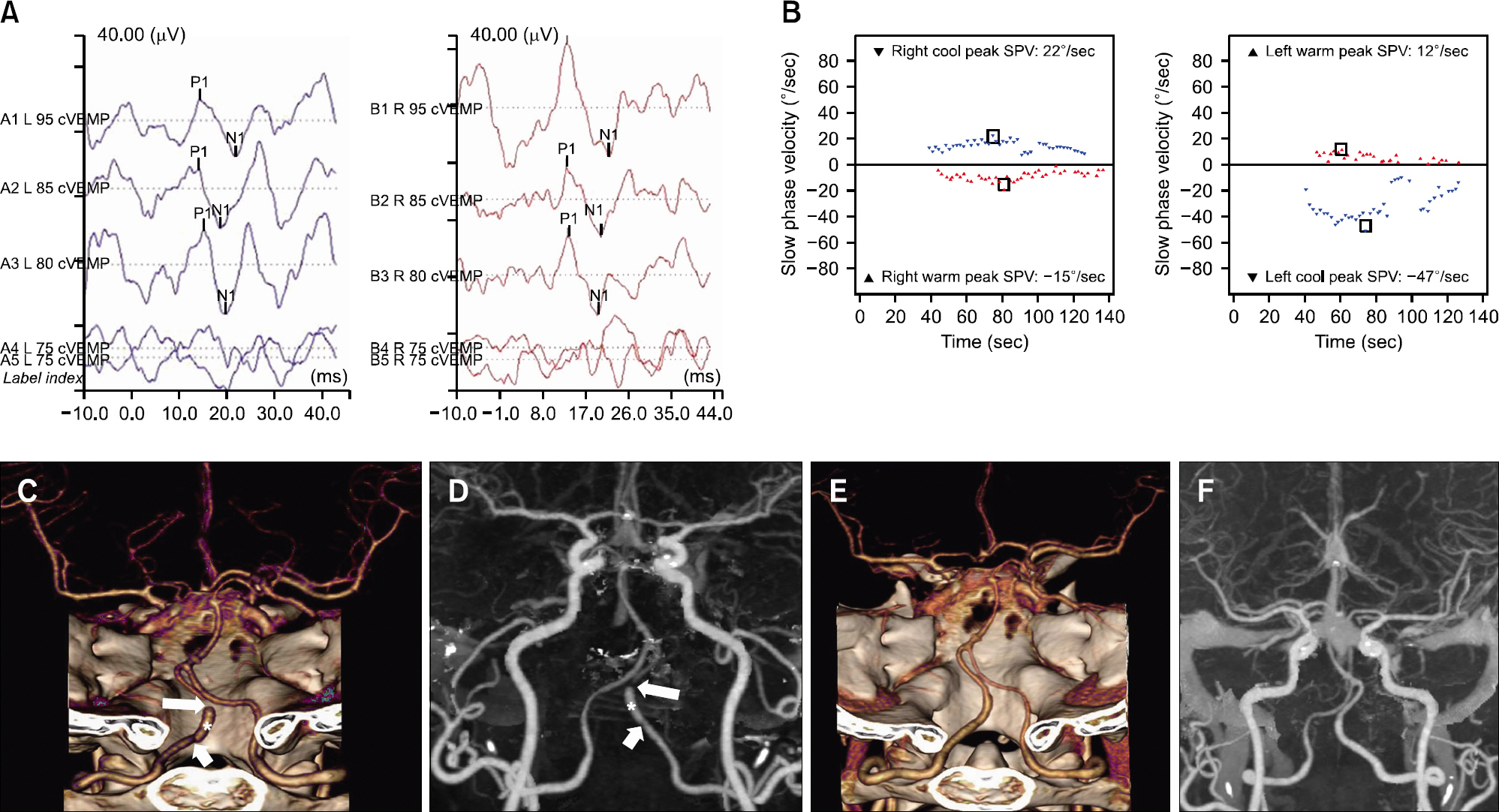
The patient was admitted to the hospital to prevent disease progression, and oral aspirin was continued to prevent stroke after discharge. The follow-up 3D-CTA, which was conducted at 2 months after the onset of dissection, revealed complete recanalization of the left vertebral artery (Fig. 1E and F).
DISCUSSION
Golf-related injuries, though golf is not a contact sport, are not uncommon with the prevalence of 25% to 62% in amateur golfers [6,7]. Although most golf-related injuries are due to overuse or trauma, devastating neurologic deficit may be resulted from cerebellar or brainstem stroke secondary to VAD. The VAD represents one of the most common causes of stroke in patients younger than 45 years old, and initiating events such as coughing, vomiting, chiropractic procedures, and blunt neck trauma may precipitate the development of the disease. Dis-section is resulted when the integrity of the arterial wall is compromised, which subsequently compromises arterial blood flow secondary to the stenosis. The vertebral artery is con-sidered highly vulnerable to mechanical stress because the vertebral artery is immobilized by the bony structures and adjacent ligaments as it passes through the transverse foramen of C6 to C1 and as it crosses the atlantoaxial segment [8]. Although VAD can be either extracranial or intracranial, oc-cipital headache or neck pain is almost always an accompanying symptom [1,2,4,5].
Our patient is the first female patient with golf swing-related VAD. She was a right-handed amateur golfer, and the dissection occurred in the intracranial segment (V4) of the left vertebral artery. Civardi et al. [4] reviewed 13 cases with golf-related VAD, which were reported in the English literature between 1990 and 2018. All 13 patients were male with the age range of 27 to 70 years. Although the handedness was unknown in 4 of 13 patients, the right VAD was more common (9 of 13 patients) than the left (3 of 13 patients) or bilateral cases (1 of 13 patients). An ischemic brain lesion was identified in the ipsilateral side of dissection in 9 of 13 patients, and the treatment outcome was excellent in most cases (12 of 13 patients). Extracranial vertebral artery was preferentially af-fected (11 of 13 patients), especially at the V2 and V3 segments [4].
It has been reported that golf-related VAD is most likely to occur on the right side and predominantly in the extracranial vertebral artery [1,2,4,5]. The junction of C1 to C2 is known to be the most common location of mechanical damage in the vertebral artery [5,8]. Because head rotation causes asymmetric forward and downward movement of the contralateral atlan-toaxial joint, the contralateral vertebral artery around the atlantoaxial joint (V3 segment) is most vulnerable to injury by head rotation [5]. A similar case of the contralateral VAD during forceful head rotation to the left was reported in a right-handed archer [9].
Choi et al. [2] postulated that because, in a right-handed golf swing, the right vertebral artery is more distant from the central axis during the body-weight shift and receives a greater torque than the left vertebral artery, the right vertebral artery is more commonly affected than the left. Yamada et al. [1] postulated that because right-handed amateur golfers often look in the direction that the ball travels from the beginning of the follow- through, the head rotates to the left rapidly with the trunk facing the front, causing damage to the right vertebral artery. However, because the motional biomechanics of a golf swing is complex involving the neck, trunk, and shoulder movements, bilateral vertebral arteries can be repetitively stretched or injured during practicing. Moreover, the location of VAD can be greatly in-fluenced by intrinsic factors such as weakness of the vessel wall or physical factors such as strength and neck length, and thus, golf-related VAD may occur at the left intracranial segment as in our patient.
It has been reported that while neck pain or occipital head-ache is always the symptom of VAD, symptoms of dizziness and nausea can develop when an ischemic lesion occurs due to dissection [10]. Imaging study showed no evidence of acute infarction in our patient, though she experienced severe vertigo, nausea, vomiting, and aggravation of the left tinnitus. The reason why our patient experienced occipital headache seven days before the development of vertigo can be explained as that VAD, which first occurred when the patient experienced oc-cipital headache, was aggravated when she felt acute vertigo during golf swing.
Interestingly, our patient showed mixed horizontal and up-beating nystagmus, which is similarly observed during head rotation in RVAO [11], even though the pathophysiology of VAD is different from that of RVAO. The RVAO is charac-terized by recurrent attacks of paroxysmal vertigo, nystagmus, tinnitus, and syncope induced by horizontal head rotation, and transient ischemia and the resulting excitation of the labyrinth in the side of the compressed vertebral artery has been proposed as a mechanism of vertigo and nystagmus [11,12]. The presence of upbeating nystagmus in our patient may be explained by ischemia of the brainstem [13], or ischemia of the vestibular end organs [12]. Considering that aggravation of ipsilesional tinnitus was accompanied by vertigo without any additional neurologic symptoms or signs typical of brainstem dysfunction, disproportionate damage to the peripheral labyrinths due to inner ear ischemia would be a plausible explanation. It has been reported that the modulation of nystagmus intensity by head position change may be resulted from an interaction between the semicircular canals and otolithic organs [14–16]. It was hypothesized that central vestibular system utilizes signals from the otolithic organs to minimize the imbalance of bilateral semicircular canals. Thus, the mechanism underlying the change in nystagmus intensity by position change in our patient can be explained similarly.
The VAD, though extremely rare, can be caused during a golf swing. Although golf-related VAD shows a generally good prognosis, high suspicion and early recognition of VAD in patients with neck or occipital headache, vertigo, and nausea would prompt early diagnosis and proper treatment.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
This work was supported by the National Research Foun-dation of Korea (NRF) grant funded by the Korea government (MSIP) (2019R1H1A1080123).
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.21790/rvs.2021.20.1.28.
REFERENCES
- 1.Yamada SM, Goto Y, Murakami M, Hoya K, Matsuno A. Vertebral artery dissection caused by swinging a golf club: case report and literature review. Clin J Sport Med 2014;24:155–7.PubMed
- 2.Choi MH, Hong JM, Lee JS, Shin DH, Choi HA, Lee K. Preferential location for arterial dissection presenting as golf-related stroke. AJNR Am J Neuroradiol 2014;35:323–6.ArticlePubMedPMC
- 3.Guptha SH, Promnitz AD, Warner A, Baron JC. A ‘collapsing’ golfer. Cerebrovasc Dis 2005;19:281–2.ArticlePubMed
- 4.Civardi C, Collini A, Genovese E, Lucchini C, Maggio M, Geda C. Vertebral artery dissection and golf swing: a paradigmatic new case. Acta Neurol Belg 2018;118:549–52.ArticlePubMed
- 5.Maroon JC, Gardner P, Abla AA, El-Kadi H, Bost J. “Golfer's stroke”: golf-induced stroke from vertebral artery dissection. Surg Neurol 2007;67:163–8.ArticlePubMed
- 6.McCarroll JR. The frequency of golf injuries. Clin Sports Med 1996;15:1–7.ArticlePubMed
- 7.Thériault G, Lachance P. Golf injuries: an overview. Sports Med 1998;26:43–57.ArticlePubMed
- 8.Showalter W, Esekogwu V, Newton KI, Henderson SO. Vertebral artery dissection. Acad Emerg Med 1997;4:991–5.ArticlePubMed
- 9.Sorensen BF. Bow hunter's stroke. Neurosurgery 1978;2:259–61.ArticlePubMed
- 10.Engelter ST, Grond-Ginsbach C, Metso TM, Metso AJ, Kloss M, Debette S. Cervical artery dissection: trauma and other potential mechanical trigger events. Neurology 2013;80:1950–7.ArticlePubMed
- 11.Park SH, Kim SJ, Seo JD, Kim DH, Choi JH, Choi KD. Upbeat nystagmus during head rotation in rotational vertebral artery occlusion. J Neurol 2014;261:1213–5.ArticlePubMed
- 12.Strupp M, Planck JH, Arbusow V, Steiger HJ, Brückmann H, Brandt T. Rotational vertebral artery occlusion syndrome with vertigo due to “labyrinthine excitation”. Neurology 2000;54:1376–9.ArticlePubMed
- 13.Pierrot-Deseilligny C, Milea D. Vertical nystagmus: clinical facts and hypotheses. Brain 2005;128(Pt 6):1237–46.ArticlePubMed
- 14.Fluur E. Interaction between the utricles and the horizontal semicircular canals. IV. Tilting of human patients with acute unilateral vestibular neuritis. Acta Otolaryngol 1973;76:349–52.ArticlePubMed
- 15.Fluur E. Integration between utricular and horizontal semicircular canal activities. Fortschr Zool 1975;23:225–34.PubMed
- 16.Fluur E, Siegborn J. Interaction between the utricles and the vertical semicircular canals. VI. Unilateral selective sectioning of the horizontal and vertical ampullar nerves, followed by tilting around the longitudinal axis. Acta Otolaryngol 1974;77:167–70.ArticlePubMed
Citations
Citations to this article as recorded by




 PubReader
PubReader ePub Link
ePub Link Cite
Cite