Abstract
- Bilateral sudden sensorineural hearing loss (SNHL) is rare, but a possible symptom of vertebrobasilar ischemia. A 69-year-old female patient with hypertension and atrial fibrillation presented with bilateral sudden hearing loss and vertigo without other neurological symptoms. On examination, she had left-beating horizontal nystagmus with positive head impulse on the left side. Pure tone audiometry revealed severe SNHL on both sides. Brain computed tomography angiography showed a dissection in the proximal portion of the basilar artery (BA) with occlusion of the mid-BA and bilateral anterior inferior cerebellar arteries (AICA), which confirmed on transfemoral cerebral angiography (TFCA). Left common carotid angiography demonstrated retrograde blood flow into the BA and right AICA via the left posterior communicating artery. During TFCA, her right hearing loss dramatically improved. Nine days later, follow-up TFCA showed an improvement of antegrade flow of the BA and AICA. We suggest that vertebrobasilar ischemia can be suspected in patients with bilateral sudden SNHL who present with risk factors for stroke.
-
Keywords: Hearing loss, Sudden; Basilar artery; Arterial dissection
-
중심단어: 돌발성난청, 기저동맥, 동맥박리
서론
돌발성난청은 이비인후과 의사가 비교적 흔하게 접하는 이비인후과적 응급질환이지만 대부분의 경우 특발성으로 발생한다. 일측으로 발생하는 경우가 흔하고 예후는 1/3 정도에서 완전히 회복되는 양상을 보인다. 하지만, 양측으로 발생하는 경우는 전체 증례의 5% 정도로 드물며 일반적으로 좋지 않은 예후를 보이고 독소, 종양, 혈관성 질환, 자가면역질환, 감염 등과 관련이 있는 것으로 알려져 있다[1]. 이 중 뇌혈관 질환의 경우 전체 환자의 1.2%에서 14.3% 정도에서 청각에 문제가 나타난다고 보고되고 있으며[2], 그 중 전하소뇌동맥(anterior inferior cerebellarartery) 영역의 뇌경색에서 청각 및 전정 증상이 발생하는 경우가 가장 흔하다[3]. 내이동맥(internal auditory artery)은 주로 전하소뇌동맥에서 분지되어 내이에 혈액을 공급하는 혈관으로, 전하소뇌동맥의 부분적인 또는 완전한 허혈에 의해 청력 손실 혹은 현훈이 단독으로 발생하기도 한다[4]. 저자들은 기저동맥(basilar artery)의 박리로 인한 양측 전하소뇌동맥의 협착으로, 다른 신경학적 증상 없이 양측 돌발성난청과 현훈만 발생한 환자를 경험하였기에 보고하고자 한다.
증례
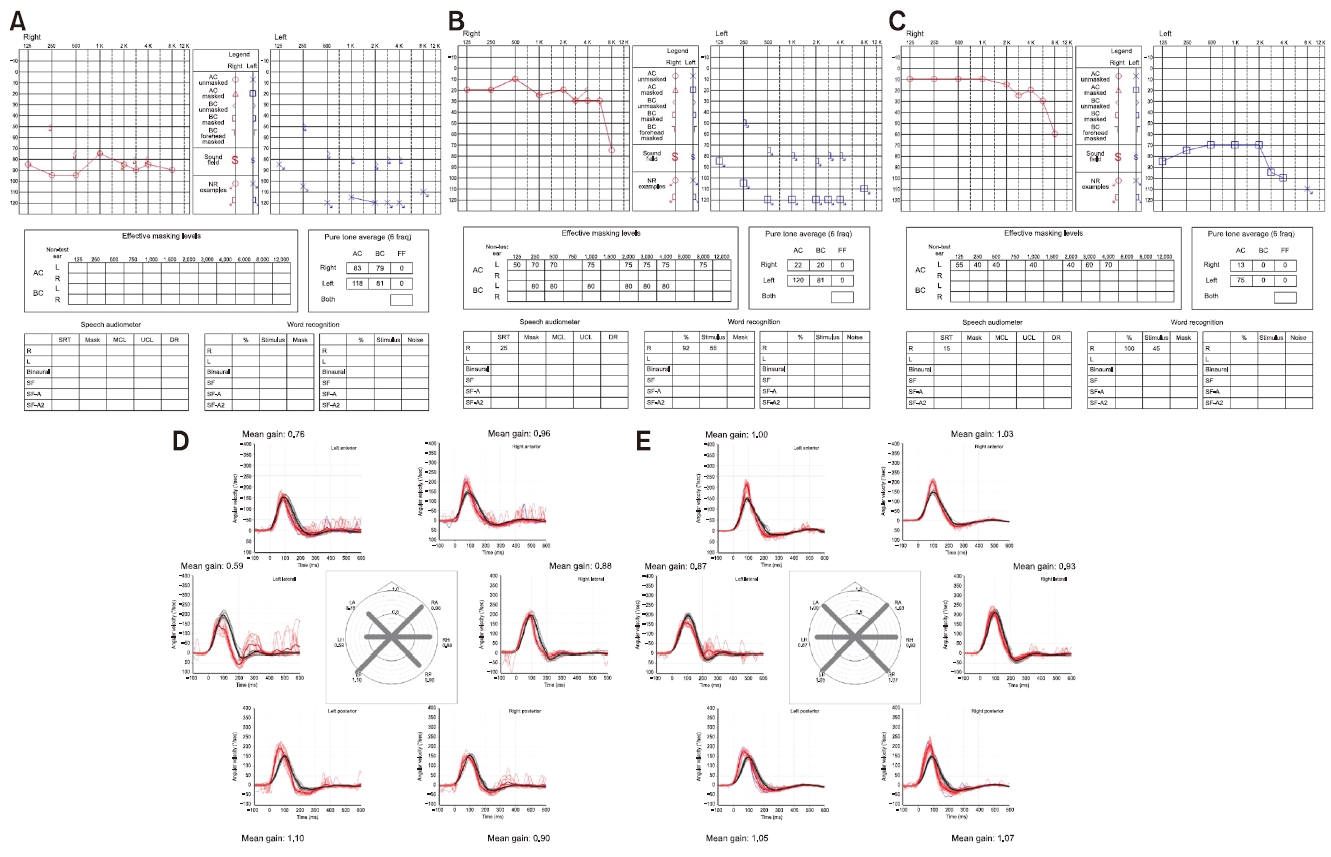
고혈압 병력이 있는 69세 여자 환자가 내원 3시간 전부터 발생한 양측 청력 저하, 이명 및 현훈으로 병원에 왔다. 환자는 동기능부전증후군(sick sinus syndrome) 및 심방 세동으로 11년 전부터 박동조율기를 삽입한 상태였고, 아스피린, 항부정맥제(flecainide), 베타차단제, 고지혈증 치료제를 복용하고 있었다. 최근 두경부 외상 병력이나 이독성 약물 복용력은 없었고, 동반되는 두통이나 경부 통증도 없었다. 이학적검사에서 양측 고막은 모두 정상이었으나, 순음청력검사에서 우측은 6분법 상으로 기도청력 역치가 83 dB, 좌측은 전농이었으며 어음명료도 검사에서 양측 0%로 확인되었다(Fig. 1A). 신경이과적 진찰에서 좌측으로 향하는 수평 자발안진이 관찰되었고, 두부충동검사 시 좌측에서 양성 소견을 보였다. 다른 신경학적 진찰에서 구음장애, 안면근육마비, 사지마비, 감각장애 및 사지실조 등은 없었다. 혈액에서 전체혈구계산, 일반혈액화 학검사, 갑상선기능검사 및 자가면역항체검사는 모두 정상이었다.
급성 현훈과 함께 양측에서 돌발성난청 소견을 보여 혈관성 원인에 대한 감별이 필요하였다. 하지만 환자는 박동조율기를 삽입한 상태로 검사 중 기기 이상으로 인한 심박동 이상이 우려되어 자기공명영상검사(magnetic resonance imaging)는 시행하지 못하였다. 뇌 컴퓨터단층촬영 (computed tomography, CT)에서 좌측 소뇌, 특히 후하소뇌 동맥 영역에 저밀도 음영이 관찰되었으며(Fig. 2A) 컴퓨터 단층혈관조영술(CT angiography)에서 기저동맥의 근위부 및 양측 척추동맥의 혈류가 확인되지 않았다(Fig. 2B). 응급으로 시행한 대퇴동맥 경유 뇌혈관조영술(transfemoral cerebral angiography, TFCA)로 좌측 척추동맥을 조영하였을 때, 양측 척추동맥이 만나는 부분 직상방까지 폐색되어 있었고, 좌측 전하소뇌동맥의 기시부는 뚜렷하게 보이지 않았으나 그 원위부는 조영되고 있어 일부 정방향 혈류(antegrade flow)는 관찰되었다(Fig. 2C, black arrowhead). 기저동맥의 원위부는 좌측 내경동맥으로부터 후교통동맥을 통해 공급받고 있었으며, 우측 전하소뇌동맥의 근위부에 혈전을 시사하는 충만결손(filling defect)이 일부 관찰되었다(Fig. 2D, white arrowhead). 우측 척추동맥 조영에서는 기저동맥의 근위부와 양측 척추동맥의 합류 지점을 포함하는 폐색으로 조영제가 기저동맥의 원위부로 진행하지 못하였다(Fig. 2E, black arrow). 뇌혈관조영술 도중 시행한 cone-beam CT에서 기저동맥 근위부 폐색과 그 내부를 채우고 있는 혈전을 좀 더 자세히 관찰할 수 있었다(Fig. 2F). 영상 소견을 종합할 때 혈관 박리에 의한 기저동맥 폐색이 의심되었다. 하지만 후교통동맥을 통한 곁순환으로 기저동맥 영역에 혈류 공급의 장애가 없었고, 검사 도중 우측 청력이 회복되는 소견을 보여 재관류치료 없이 시술을 마쳤다.
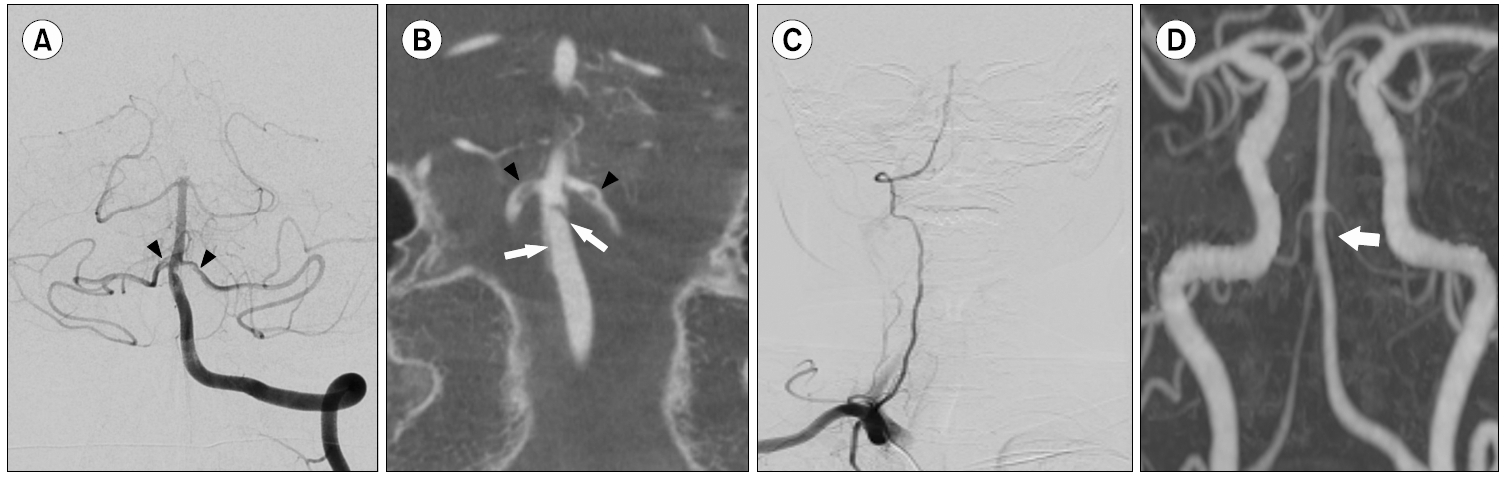
입원 이후 환자의 어지럼은 점점 호전되었고, 뇌혈관 조영술 다음날에 시행한 순음청력검사에서 우측은 평균 청력역치가 22 dB로 호전되었으나 좌측은 여전히 전농 상태였으며, 어음명료도는 우측 92%, 좌측 0%로 확인되었다(Fig. 1B). 비디오안진검사에서는 이전에 좌측으로 향하던 수평 자발안진이 우측으로 방향이 바뀌었으며 온도 안진검사에서는 좌측 반고리관마비(54%), 비디오두부충동검사에서 좌측 수평반고리관 자극 시 이득 저하(0.59; 정상, 0.87–1.04)와 함께 현성신속안구운동(overt saccade)이 관찰되었다(Fig. 1D). 입원 후 9일째에 재시행한 뇌혈관조 영술에서 좌측 척추동맥 조영 시 정방향 혈류가 완전히 회복되었으며(Fig. 3A) 기저동맥 근위부에 불규칙한 모양의 피판이 관찰되어 본 환자의 진단이 혈관 박리임을 확인할 수 있었다(Fig. 3B). 내막판은 양측 전하소뇌동맥의 기시부까지 이어져 있었으며 일부 남아있는 혈관벽 내 혈전이 충만결손의 형태로 보이고 있었다(Fig. 3B, black arrowhead). 기저동맥 근위부 폐색의 재개통으로 인해 우측 척추동맥을 조영하였을 때에도 정방향 혈류가 되살아난 것을 볼 수 있었다(Fig. 3C).
환자는 2주간 하루 한 번 경구용 항혈소판제 3제요법 (aspirin 100 mg+cilostazol 200 mg+clopidogrel 75 mg)을 시행한후, 경구용 항응고제(edoxaban 30 mg)와 항혈소판제(cilostazol 200 mg) 병용요법으로 변경하였다. 다만 일반적으로 특발성 돌발성난청에서 시행하는 고용량 스테로이드 치료는 환자의 난청 원인이 혈관성인 것으로 판단되어 시행하지 않았다. 퇴원 당시 어지럼은 모두 호전되어 자발안진은 관찰되지 않았고, 비디오두부충동검사의 이득도 정상화 되었지만(Fig. 1E) 좌측 청력은 회복되지 않았다. 퇴원 1개월 뒤 재시행한 컴퓨터단층혈관조영술에서는 기저동맥이 정상화되었고, 양측 전하소뇌동맥도 잘 관찰되었다 (Fig. 3D). 퇴원 6개월 뒤 재시행한 청력검사에서 우측 청력역치는 13 dB, 좌측 청력역치는 75 dB 로 좌측 청력이 일부 회복된 것이 관찰되었으며, 어음명료도는 우측 100%, 좌측 0%로 확인되었다(Fig. 1C).
고찰
양측 돌발성난청은 전체 돌발성난청의 5% 미만을 차지하지만, 전신질환과 연관이 있는 경우가 많고 예후가 좋지 않기 때문에 빠른 진단과 치료가 필요하다[1]. 본 증례의 경우 과거력에서 난청을 일으킬 만한 원인은 없었고 혈액검사에서도 특별한 이상은 발견되지 않았다. 박동조율기를 삽입한 상태로 뇌 자기공명영상검사는 시행할 수없었지만, 응급 뇌혈관조영술을 통해 기저동맥 박리 및폐색으로 인한 양측 돌발성난청을 진단할 수 있었다.
돌발성난청의 원인으로 척추기저동맥의 폐색은 전체 원인 중 약 1.2%를 차지할 정도로 드문 질환이다[2]. 또한 척추기저동맥 폐색의 약 1.4%에서만 양측 돌발성난청이 발생하는 것으로 보고되고 있다[5]. 이렇게 척추기저동맥 폐색에서 돌발성난청과 현훈이 발생하는 이유는 전하소 뇌동맥에서 기원하는 내이동맥의 허혈 때문이다. 전하소 뇌동맥은 와우핵, 위 및 내측 전정핵, 7번 및 8번 뇌신경 및 그 근위부의 혈류를 담당함과 동시에 내이에 분포하는 주된 혈관인 내이동맥의 주된 공급원이다[6]. 특히 내이는 많은 에너지 대사를 요구하는 기관이지만, 내이동맥은 전하소뇌동맥의 말단 동맥이면서 측부 순환이 발달하지 않았기 때문에 다른 후미로성 구조물에 비해 허혈에 취약하다[4]. 따라서 기저동맥 폐색 시 전하소뇌동맥이 함께 침범되면 내이동맥 경색에 의해 내이 기능 장애가 발생할수 있다. 본 증례에서도 뇌혈관조영술에서 기저동맥의 폐색과 함께 양측 전하소뇌동맥의 근위부에 협착이 확인되 었기 때문에, 이로 인한 내이동맥의 혈류 장애로 현훈과 양측 돌발성난청이 발생했을 것으로 여겨진다. 하지만 전하소뇌동맥의 원위부 혈류는 유지되고 있었기 때문에 기저동맥 또는 후하소뇌동맥(posterior inferior cerebellar artery) 폐색으로 양측 돌발성난청이 발생했을 가능성도 배제할 수 없다. 즉 내이동맥은 대부분 전하소뇌동맥에서 기원하지만, 일부는 후하소뇌동맥이나 기저동맥에서 직접 기원하기도 때문이다[7].
기저동맥이 폐색된 환자들은 대부분 뇌간과 소뇌의 광범위한 경색으로 인해 사지 위약감이나 실조증, 감금증후군(locked-in syndrome), 의식저하 등과 같은 심각한 신경학적 증상을 보이기 때문에 돌발성난청만 양측으로 발생하는 경우는 매우 드물다[8,9]. 본 증례에서는 기저동맥 박리로 근위부가 폐색되었지만, 후교통동맥을 통해 좌측 내경동맥으로부터 기저동맥 원위부로 혈류를 공급받고 있어 현훈과 양측 난청 외에 다른 신경학적 증상은 나타나지 않았다. 특히 우측 전하소뇌동맥은 근위부 협착에도 불구하고 내경동맥으로부터 들어오는 혈류가 좋은 상태였기 때문에 우측 청력이 빠르게 호전되었다. 이에 반해 좌측 전하소뇌동맥은 근위부 협착이 심한 상태로 내경동맥으로부터 혈류를 공급받지 못하여 좌측 청력과 전정기능은 회복되지 못했을 것으로 여겨진다. 이후 기저동맥 박리가 호전되면서 기저동맥과 전하소뇌동맥의 혈류도 정상화되었지만, 좌측 청력저하는 지속되고 있는 상태이다.
돌발성난청이 양측에서 발생할 경우 대부분 예후가 좋지 않기 때문에 원인 질환에 대한 빠른 진단과 치료가 필요하다. 특히 뇌혈관 질환의 위험인자를 가진 고령의 환자에서 현훈과 함께 양측 청력저하가 발생한 경우 비록 전형적인 뇌간 및 소뇌 증상을 보이지 않더라도 반드시 척추기저영역(vertebrobasilar territory)의 허혈성 손상을 염두에 두어야 한다.
ARTICLE INFORMATION
-
저자들은 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.
Fig. 1.Changes in the results of pure tone audiometry (PTA) and video head impulse test (vHIT). (A) Initial PTA shows symmetrical bilateral hearing loss. (B) PTA after computed tomography angiography reveals that right hearing loss was improved, but left hearing loss still persisted. (C) At 6 months follow-up PTA, left hearing loss was partially improved. (D) Initial vHIT shows decreased vestibulo-ocular reflex (VOR) gain with overt saccades in left horizontal semicircular canal (normal gain, 0.87–1.04). (E) At 7-day follow-up vHIT, the VOR gain for left horizontal semicircular canal was nearly normalized.
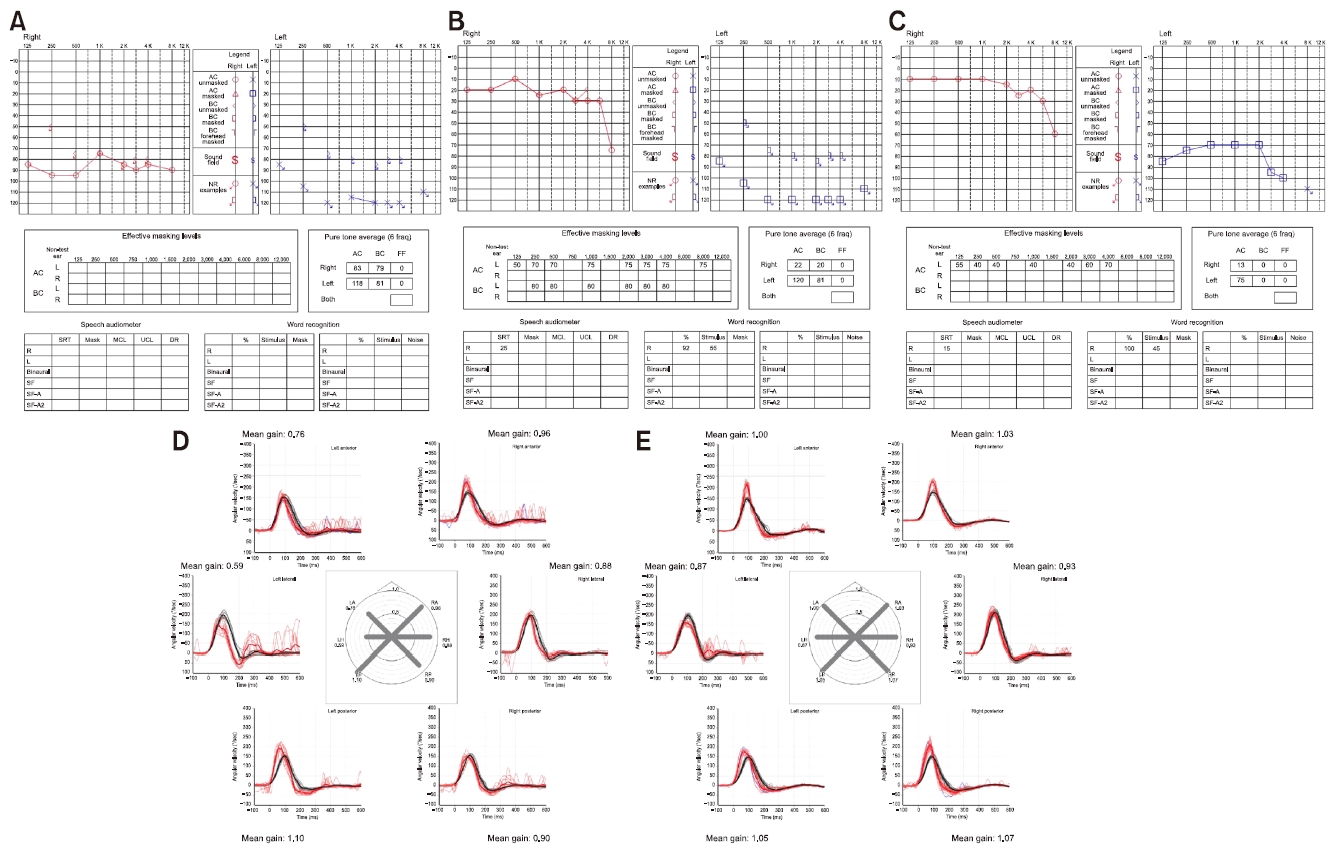
Fig. 2.Brain computed tomography (CT) and angiographic findings at the initial presentation. (A) Axial noncontrast enhanced brain image shows subtle hypodense area (white arrow) in left cerebellum. (B) On CT angiography with maximum intensity projection reconstruction image, distal segments of both vertebral artery (VA) (white arrow) and proximal basilar artery (BA) (white arrowhead) are not visible, but distal BA is opacified probably from collateral flow via left posterior communicating artery (P-com). (C) Transfemoral cerebral angiography shows occlusion and filling defect of the proximal BA (white arrow) and the origin of left anterior inferior cerebellar artery (AICA, black arrowhead). (D) Blood flows of the distal BA and right AICA were maintained from left carotid artery through P-com. In the proximal portion of right AICA, there is filling defect due to suspicious thrombus (white arrowhead). (E) The fourth segment of right VA was not identified due to BA occlusion (black arrow). (F) Cone-beam CT image during angiography shows a filling defect in the proximal BA.
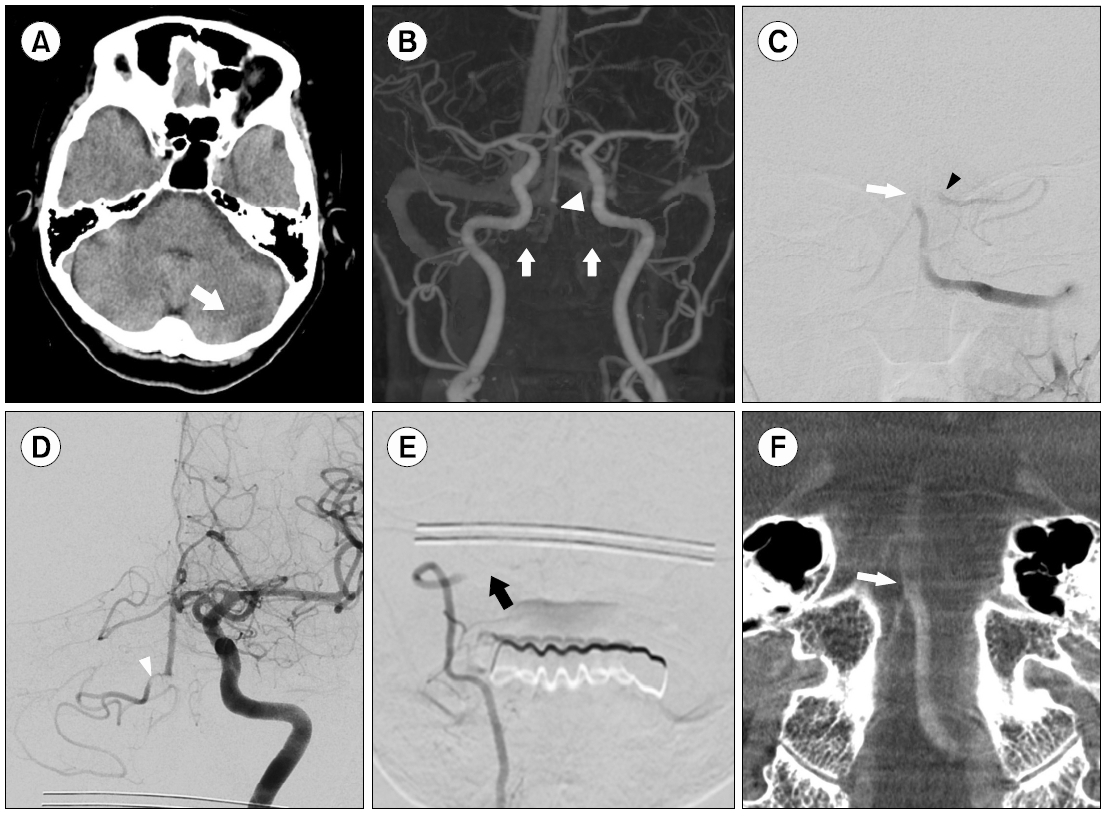
Fig. 3.Follow-up computed tomography (CT) and angiography images. (A) Follow-up cerebral angiography after 9 days of hospitalization shows a reappearance of antegrade flow of basilar artery (BA) and both anterior inferior cerebellar artery (AICA), but some filling defects caused by thrombus and vessel flap in the proximal portion of AICA (black arrowheads). (B) Cone-beam CT image after nine days of hospitalization reveals linear low-density structures (white arrows), which are considered as flaps. There are also filling defects caused by thrombus and flap in the proximal portion of both AICA (black arrowheads). (C) The antegrade flow of right vertebral artery was identified. (D) Follow-up CT angiography after 1 month shows a normalization of blood flows of BA and both AICAs (white arrow).

REFERENCES
- 1. Sara SA, Teh BM, Friedland P. Bilateral sudden sensorineural hearing loss: review. J Laryngol Otol 2014;128 Suppl 1:S8–15.ArticlePubMed
- 2. Sauvaget E, Kici S, Petelle B, Kania R, Chabriat H, Herman P, et al. Vertebrobasilar occlusive disorders presenting as sudden sensorineural hearing loss. Laryngoscope 2004;114:327–32.ArticlePubMed
- 3. Lee H, Sohn SI, Jung DK, Cho YW, Lim JG, Yi SD, et al. Sudden deafness and anterior inferior cerebellar artery infarction. Stroke 2002;33:2807–12.ArticlePubMed
- 4. Perlman HB, Kimura R, Fernandez C. Experiments on temporary obstruction of the internal auditory artery. Laryngoscope 1959;69:591–613.ArticlePubMed
- 5. Huang MH, Huang CC, Ryu SJ, Chu N S. Sudden bilateral hearing impairment in vertebrobasilar occlusive disease. Stroke 1993;24:132–7.ArticlePubMed
- 6. Han Z, Leung TW, Lam W, Soo Y, Wong KS. Spontaneous basilar artery dissection. Hong Kong Med J 2007;13:144–6.PubMed
- 7. Lee H, Baloh RW. Sudden deafness in vertebrobasilar ischemia: clinical features, vascular topographical patterns and long-term outcome. J Neurol Sci 2005;228:99–104.ArticlePubMed
- 8. Kim E, Son MK, Kang CK, Lee YB. Vertebrobasilar occlusion presenting as sudden isolated bilateral sensorineural hearing loss: case report. J Cerebrovasc Endovasc Neurosurg 2013;15:225–8.ArticlePubMedPMC
- 9. Kinouchi T, Ishitani K, Uyama S, Miyamoto T, Fujimoto N, Ueta H. Basilar artery occlusion presenting as sudden bilateral deafness: a case report. J Med Case Rep 2021;15:111. ArticlePubMedPMC
Citations
Citations to this article as recorded by




 PubReader
PubReader ePub Link
ePub Link Cite
Cite