돌발성난청환자에서 양성돌발성두위현훈 발현의 예후는?
What Is the Prognosis of Patients with Benign Paroxysmal Positional Vertigo in Sudden Sensorineural Hearing Loss?
Article information
Trans Abstract
Objectives
Vertigo is considered a poor prognostic factor in patients with sudden sensorineural hearing loss (SSNHL). Benign paroxysmal positional vertigo (BPPV) is a common cause of vertigo and may accompany SSNHL. However, whether BPPV is a poor prognostic factor remains controversial. We identified features of prognostic utility in patients with both SSNHL and BPPV.
Methods
We retrospectively evaluated data on all patients diagnosed with SSNHL at Keimyung University Dongsan Medical Center between January 2011 and December 2015. We reviewed medical records, the results of vestibular function testing, and audiographic data.
Results
Of the 524 idiopathic SSNHL patients, 20 (3.8%) were also diagnosed with unilateral BPPV. The average pure tone average (PTA) of those with both SSNHL and BPPV was higher than that of those without BPPV. Of the 471 patients with SSNHL only, 143 (30%) exhibited complete recovery. Of the 33 SSNHL patients with vertigo, 3 (9%) exhibited complete recovery, but only 3 (15%) of those with both SSNHL and BPPV exhibited complete recovery. Of the 20 patients with both SSNHL and BPPV, 15 had ipsilateral BPPV and 5 contralateral BPPV.
Conclusions
Patients with BPPV had a higher average initial PTA score and poorer hearing recovery after treatment, than patients with SSNHL alone. Patients with contralateral BPPV had a somewhat better prognosis than those with ipsilateral BPPV, but statistical significance was not attained.
INTRODUCTION
Sudden sensorineural hearing loss (sudden SNHL) is defined as a loss ≥30 dB at ≥3 continuous frequencies within 72 hours [1]. The annual incidence of sudden SNHL ranges from 5 to 20 cases per 100,000 individuals in the USA [2]. Although neither the pathophysiology nor the cause of sudden SNHL has been fully determined, several factors are considered to affect recovery [3]. Such factors include the initial extent of hearing loss, the interval from sudden SNHL onset to treatment, age, the type of hearing loss, and vertigo [2,4-6]. The proportion of sudden SNHL accompanied by vertigo is 40%–60% [7-10]. Vestibular symptoms may reflect injury to the labyrinth or the eighth cranial nerve; concurrent vertigo is negatively prognostic [11].
Park et al. [12] reported that peripheral vestibulopathy was a useful prognostic factor in those with sudden SNHL; however, the prognostic significance of BPPV remains controversial. Here, we explore the association between recovery and BPPV status of sudden SNHL patients.
MATERIALS AND METHODS
We retrospectively reviewed charts of patients who were diagnosed with sudden SNHL from January 2011 to December 2015 at Keimyung University Dongsan Medical Center.
Criteria of sudden SNHL includes hearing loss over 30 dB in more than 3 consecutive frequency in a pure tone audiogram in three days.
We excludes patients with delayed treatment over 2 weeks. Patients who had previous trauma or otologic surgery history or ototoxic drug use history were excluded too. All patient took brain magnetic resonance imaging and then cerebral lesion or vestibular shcwannoma were excluded.
Pure tone audiogram (PTA) was done at first visit and follow up pure tone audiogram were performed a week, a month and 3 months later. The PTA average was defined average hearing threshold at 500, 1 k, 2 k, 3 k Hz (AAO-HN) [13]. All patients were treated for sudden SNHL with prednisone (1 mg/kg/day, 12 days, tapering regimen). We compared first audiogram with 3 months later audiogram to analyze recovery.
To evaluate vertigo, every patients had vestibular function test at first visit.
Test includes spontaneous nystagmus, gaze nystagmus, head shaking and vibration nystagmus, positional nystagmus (Dix- Hallpike test, head rolling test). Video eye movement recording system (SLVNG, SLMed, Seoul, Korea) was used.
The patients who complaint dizziness when they experience difficulties in hearing were suspected of subjective vertigo.
Patients were divided three groups which include sudden SNHL only, sudden SNHL with BPPV, sudden SNHL with vertigo.
BPPV group includes patients who were suffered from any type of BPPV within 2 weeks after occurring sudden SNHL. Vertigo group means every patient who had subjective vertigo with vestibular hypofunction but without BPPV.
Head shaking test, head impulse test and caloric test were used to diagnosis the vestibular hypofunction.
The degree of hearing recovery was evaluated base on the Siegel’s criteria (complete recovery: final hearing better than 25 dB, Partial recovery: more than 15 dB gain, final hearing 25 to 45 dB, Slight improvement: more than 15 dB gain, final hearing poorer than 45 dB, No improvement: less than 15 dB gain, final hearing poorer than 75 dB) [14].
In this study, complete recovery and partial recovery were assigned to good recovery, slight improvement and no recovery were assigned to poor recovery.
Statistical analyses were performed with the SPSS software ver. 22.0 (SPSS Inc., an IBM company, Chicago, IL, USA) using independent t-test, pearson chi-square test, one way analysis of variance. A p-value <0.05 means statistically significant.
RESULTS
There are 524 patients who were diagnosed with sudden SNHL. 20 patients of them were suffered from BPPV. 33 patients had subjective vertigo and showed abnormal vestibular function. Average age were 56.4 years old. Of 524 patients, 258 patients were males and 266 were females. There were no statistical significance in average age and sex ratio among the three groups (sudden SNHL only, sudden SNHL with BPPV, sudden SNHL with vertigo) (Table 1).

Characteristics of patients who had sudden sensorinueral hearing loss
Twenty patients had diverse BPPV types. Interestingly, 5 patients showed BPPV on opposite side ear (contralateral BPPV). Whirling vertigo symptom of contralateral BPPV attacked on the same day when they felt sudden hearing difficulty. There was no difficulty in diagnosing BPPV.
All of five contralateral BPPV were lateral canal type. 3 cases were geotrohpics and 2 cases were apogeotropics.
Another 15 BPPV cases occurred on the same side ear with sudden SNHL. The posterior canal type were 6 cases and geotropic lateral canal were 5, apogeotropic lateral canal were 4 (Table 2, Fig. 1).

Subtypes of BPPV
The proportion of benign paroxysmal positional vertigo types.
The Patients who had ipsilateral BPPV showed worse average PTA than the contralateral BPPV patients. In the case of ipsilateral BPPV, initial average PTA was 88.2 dB and after 3 months later post treatment average PTA was 73.5 dB. The initial average PTA of contralateral BPPV was 80.2 dB and post treatment was 58.2 dB. There was even more difference in post treatment PTA, but no statistically significant difference (Fig. 2).
Comparison of average PTA between ipsilateral BPPV and contralateral BPPV. PAT, pure tone average; BPPV, benign paroxysmal positional vertigo.
Compared with sudden SNHL only group, patients with ipsilateral side BPPV and with subjective vertigo were reported worse initial average PTA and post treatment average PTA. These difference has statistical significance (p<0.05). The initial average PTA of sudden SNHL only group was 68.9 dB, and group with ipsilateral BPPV was 88.2 dB, group with subjective vertigo was 77.4 dB.
The post treatment average PTA of sudden SNHL only group was 43.6 dB and 73.5 dB for BPPV group and 63.2 dB for subjective vertigo group (Fig. 3). Groups who had ipsilateral BPPV and subjective vertigo showed statistically significant better initial PTA and post treatment PTA than sudden SNHL only group. But there was no statistical significance between ipsilateral BPPV group and vertigo group.

Change of the average PTA between initial visit and post treatment (post Tx: 3 month later). (A) Patients group who had BPPV shows poorer initial PTA and post treatment PTA than sudden SNHL only group. (B) Patients group who had sudden SNHL with vertigo shows poorer initial PTA and poorer post treatment (post Tx: 3 month later) PTA than sudden SNHL only group. both (A), (B) had statistically significant (p<0.05). PAT, pure tone average; BPPV, benign paroxysmal positional vertigo; SNHL, sensorineural hearing loss.
Sudden SNHL only group showed high proportion of complete recovery (n=143, 30.4%) compared with other groups. BPPV group showed high proportion of no improvement (n=7, 35.0%) and slight improvement (n=8, 40.0%), vertigo group showed high no improvement (n=16, 48.4%) proportion too (Table 3).
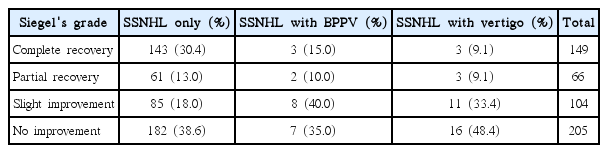
Recovery proportion of three groups according to Siegel’s criteria
In the case of good recovery, there is statistical difference between sudden SNHL group and BPPV group or subjective vertigo group but there was no statistic difference between BPPV and subjective vertigo groups (Table 4).

Comparison of recovery prognosis
DISCUSSION
Vertigo is known to be poorly prognostic, but commonly encountered in sudden SNHL patients [15]. Vertigo is not a disease, but rather a symptom; our focus was on BPPV, which commonly causes peripheral vertigo accompanied by sudden SNHL. BPPV could cause by migration of otoloith into semicircular canals, it might be a factor that means severe labyrinth damage [11]. Thus, sudden SNHL patients with BPPV may exhibit more severe labyrinth damage associated with poorer recovery then we could suppose that these patients would show poor recovery.
Hypoperfusion of the inner ear, thought potentially to cause sudden SNHL in patients under prolonged cardiopulmonary bypass therapy, may also explain the sudden SNHL of BPPV patients [16,17]. Baloh and Honrubia [18] found that vascular occlusion of the inner ear caused the release of otoconia from macular utricles. Transient labyrinthine ischemia may trigger patchy loss of inner ear function, associated with sudden SNHL and BPPV/vertigo [17].
Viral infection may also trigger sudden SNHL combined with BPPV, inflaming and damaging the labyrinth, accompanied by vestibulopathy and Bell’s palsy [19,20]. Karlberg et al. [20] considered that viral infection of the labyrinth might trigger BPPV.
We studied 20 patients (3.8% of the total) with both sudden SNHL and BPPV. Of these, 15 (2.9%) exhibited BPPV on the same side as hearing loss and 5 (0.1%) BPPV on the other side. All contralateral BPPV attacks developed within 24 hours after sudden SNHL. BPPV diagnosis was not difficult.
In the case of contralateral ear BPPV, exact pathophysiology and effect on hearing loss were out of scope in our study.
It is possible that viral infection may affect the contralateral ear, triggering BPPV. But we couldn’t rule out the possibility of accident event. It is difficult to confirm the exact pathophysiology.
Sudden SNHL with BPPV groups clearly exhibited poorer initial hearing and recovery than sudden SNHL only group.
Compared to contralateral BPPV group, ipsilateral BPPV group had poorer initial hearing and recovery result, but there were no statistical significant.
We supposed that ipsilateral BPPV could be a worse prognosis factor than contralateral BPPV, but statistical significant were insufficient to reach that conclusion.
The group with BPPV and vertigo had poor recovery than the sudden SNHL only group. All of these factors which including BPPV or vestibulopathy (vertigo group) could indicate worse initial PTA result too.
The initial hearing threshold is undisputed prognostic factor in hearing outcome [21]. We thought that BPPV may reflect more severe labyrinthine damage, so could induce poor initial hearing. Then it could become a poor prognosis factor. It is already known that sudden SNHL patients with vestibulopathy (sudden SNHL with vertigo group) have a poor prognosis.
Lateral semicircular canal type BPPV was more common in sudden SNHL patients with BPPV [10]. However, we found no significant difference among BPPV types. Lee and Ban [22] reported that subtypes of BPPV couldn’t influence on the hearing outcome, just reflect serious labyrinthine damage on canals.
In conclusion, BPPV may be poorly prognostic of sudden SNHL associated with severe, widespread labyrinthine damage which could indicate worse initial hearing. Further research is needed for pathophysiology and relationship with contralateral BPPV.
Notes
No potential conflict of interest relevant to this article was reported.