수평반고리관 양성돌발두위현훈에서의 가성자발안진과 두진후안진
Pseudo-Spontaneous Nystagmus and Head-Shaking Nystagmus in Horizontal Canal Benign Paroxysmal Positional Vertigo
Article information
Trans Abstract
Objectives
The purpose of this study was to examine the clinical manifestations and significance of pseudo-spontaneous nystagmus (PSN) and head-shaking nystagmus (HSN) in horizontal canal benign paroxysmal positional vertigo (HC-BPPV).
Methods
Two hundred fifty-two patients diagnosed as HC-BPPV were reviewed retrospectively. After excluding 55 patients with ipsilateral vestibular diseases, multiple canal BPPV, or those who were lost to follow-up, we analyzed the direction of PSN and HSN in patients with HC-BPPV. We also compared the clinical characteristics and treatment outcome between PSN-positive and PSN-negative groups.
Results
Our study included 197 patients composed of 80 patients with geotropic HC-BPPV and 117 patients with apogeotropic HC-BPPV. PSN was observed in 13.7% patients and HSN was observed in 45.2%. The incidence of HSN was higher in apogeotropic HC-BPPV, while the proportion of PSN was not statistically significant between the two subtypes. There was no directional preponderance in geotropic HC-BPPV, while ipsilesional PSN and contralesional HSN showed higher incidence in apogeotropic HC-BPPV. The dizziness handicap inventory score in the PSN-positive group was higher than that in the PSN-negative group (p<0.001), and the duration of symptom onset in the PSN-positive group was shorter than that in the PSN-negative group (p=0.047). However, there was no significant difference in the treatment outcome between the two groups.
Conclusions
The incidence of HSN was higher than that of PSN in patients with apogeotropic HC-BPPV. Patients with HC-BPPV showing PSN demonstrated more severe initial symptoms and visited the hospital in a shorter period of time after the onset of symptoms.
서 론
양성돌발두위현훈(benign paroxysmal positional vertigo, BPPV)은 자세 변화에 따라 반복적으로 나타나는 회전성 어지럼을 특징으로 하는 가장 흔한 말초성 전정질환이다[1,2]. BPPV는 일반적으로 자발안진이 관찰되지 않으며, 체위검사를 통해 유발되는 특징적인 안진을 동반하는 회전성 어지럼을 통해 진단한다. BPPV에서 이환되는 각 반고리관 아형과 이환된 귀를 결정하기 위해 Dix-Hallpike 수기와 누워머리돌리기검사(supine head roll test)의 사용을 권장하고 있으며[3,4], 수평반고리관 BPPV (horizontal canal BPPV, HC-BPPV)에서 이환된 귀를 결정하기 어려운 경우 Bow and lean test를 보조적인 진단방법으로 사용한다[5]. 최근 HC-BPPV에서 보이는 자발안진과 두진후안진에 대한 연구들이 발표되고 있는데, 2015년 Barany 학회에서 제시한 BPPV의 진단기준에서는 HC-BPPV에서 관찰되는 자발안진을 ‘가성자발안진(pseudo-spontaneous nystagmus)’이라고 소개하고 있으며[4,6,7], 수평반고리관이 수평면에서 30도 정도 위를 향하는 해부학적 구조로 인해 발생하는 것으로 보고되고 있다[6-9]. 이전 연구들에서 가성자발안진의 발생 빈도는 15%–76%, 두진후안진의 빈도는 30%–96%로 다양하게 보고되고 있으며[6-9], 일부 연구에서는 가성자발안진이나 두진후안진의 방향을 HC-BPPV의 이환된 귀방향 결정에 참조할 가치가 있다는 보고도 있다[8,9]. 이에 저자들은 HC-BPPV 환자들에서 가성자발안진과 두진후안진의 발현율을 확인하여 이들 소견의 임상적 의미를 살펴보고, 이들 소견 중 가성자발안진의 유무에 따라 BPPV의 임상양상이나 치료율에 차이가 있는지 확인해보고자 하였다.
대상 및 방법
2010년 1월부터 2013년 1월까지 본원 이비인후과로 내원한 HC-BPPV로 진단된 252명의 환자들을 대상으로 후향적으로 설문지 및 의무기록을 검토하였다. 모든 환자에서 가성자발안진 및 두진후안진을 확인하였고, 신경학적 검사를 통해 중추 신경계의 질환 여부를 확인하였다. 연구의 대상이 된 환자들 중 BPPV가 여러 반고리관에 이환된 환자, BPPV에 영향을 줄 수 있는 다른 귀 질환(만성 중이염, 전정신경염, 돌발성 난청, 메니에르병)을 병변측에 함께 갖고 있는 환자, 그리고 검사에 협조적이지 못하거나 외래추적 관찰이 이루어지지 못한 환자들 등 총55명은 연구 대상에서 제외하였다.
BPPV의 진단은 2008년 미국 이비인후과학회에서 제시한 진료 지침에 따라 Dix-Hallpike 수기와 누워머리돌리기 검사를 통해 각 이환된 반고리관을 결정하였다[3]. 안진의 확인은 video Frenzel goggle system (SLMED, Seoul, Korea)을 사용하였다. HC-BPPV의 아형과 이환된 방향은 다음 검사에 의해 유발된 안진에 따라 분류하였다. HC-BPPV의 향지성 아형(geotropic HC-BPPV, HC-BPPV [Geo])은 누워머리돌리기검사에서 전형적인 향지성 방향의 방향변환성 체위안진(direction changing positional nystagmus, DCPN)을 확인하고 누워머리돌리기검사에서 강한 안진을 나타내는 방향을 병변측으로 진단하였다. HC-BPPV의 원지성 아형(apogeotropic HC-BPPV, HC-BPPV [Apo])은 누워머리돌리기검사에서 전형적인 원지성 방향의 DCPN을 확인하고, 약한 안진이 유발되는 방향을 병변측으로 진단하였다. HC-BPPV의 2가지 아형을 진단할 때, 양측 안진의 세기가 같은 경우에는 머리숙임-젖힘검사(bow and lean test)를 통해 병변의 방향을 결정하였다[5].
BPPV의 치료는 HC-BPPV (Geo)의 경우 modified Lempert maneuver를 시행하였고, HC-BPPV (Apo)의 경우 new cupulolith repositioning maneuver를 시행하였다[10]. 치료는 진단 당일 1회의 치료를 시행하고, 다음 방문 시 내원하여 재평가하는 방식으로, 치료 성공 시까지 매 방문 시 1회씩 치료하였다. 치료의 성공은 재방문 시 시행한 체위검사에서 특징적인 안진이 관찰되지 않으면서 체위현훈이 사라진 경우로 정의하였다.
가성자발안진이 보이는 군과 보이지 않는 군 간의 임상양상을 나이, 성별, 어지럼 발생부터 진단 시점까지의 기간, dizziness handicap inventory (DHI) 점수 별로 나누어 분석하였다. 또한, HC-BPPV의 아형에 따른 가성자발안진의 발생 빈도와 두진후안진의 발생빈도를 확인하고, 각 아형에 따른 가성자발안진의 발생 빈도 차이와 두진후안진의 발생 빈도 차이에 대한 상관관계는 각각 χ2 test를 통해 분석하였다. 그리고 각 아형 내에서 가성자발안진의 방향에 따른 빈도의 차이와 두진후안진의 방향에 따른 빈도의 차이를 각각 Binomial test를 통해 분석하였다. 또한 HC-BPPV환자에서 가성자발안진이 보이는 군과 보이지 않는 군 간의 임상양상 및 치료 결과의 상관관계를 확인하기 위해 Independent t-test, Mann-Whitney U test, χ2 test를 통해 분석하였다. 통계학적 분석은 PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA)을 사용하였으며, p값이 0.05 미만일 때 통계적으로 유의하다고 판정하였다.
결 과
본 연구의 대상이 된 HC-BPPV 환자 197명 중 남자가 52명(26%), 여자가 145명(74%)이었고, 평균 연령은 53.1±15.2세 (범위, 13–89세)였다. HC-BPPV 환자의 아형에 따른 분포를 살펴보면, HC-BPPV (Geo) 환자는 80명(40.6%), HC-BPPV(Apo) 환자는 117명(59.4%)이었다. HC-BPPV 환자 197명중 가성자발안진이 보이는 환자는 27명(13.7%), 두진후안진이 보이는 환자는 89명(45.2%)이었다.
HC-BPPV 환자에서 두 아형 간 가성자발안진의 발생 빈도는 유의한 차이를 보이지 않았으나(p=0.094), 두진후안진은 HC-BPPV (Apo)에서 51.3%로 HC-BPPV (Geo)의 36.2% 보다 높은 빈도로 나타났다(p=0.037) (Table 1).
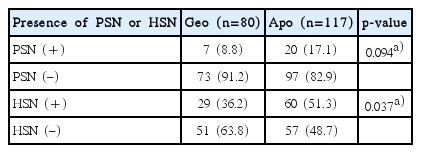
Distribution of patients according to the presence of PSN and HSN in geotropic and agpogeotropic subtypes of horizontal canal benign paroxysmal positional vertigo
HC-BPPV (Geo)에서 가성자발안진의 방향에 따른 발생빈도는 유의한 차이를 보이지 않았으나(p=0.453), HC-BPPV(Apo)에서는 가성자발안진의 방향에 따라 발생빈도에 유의한 차이를 보였으며, 주로 병변측으로 향하는 경우가 많았다(p=0.041) (Fig. 1). 또한 HC-BPPV (Geo)에서 두진후안진의 방향에 따른 발생빈도는 유의한 차이를 보이지 않았으나(p=0.136), HC-BPPV (Apo)에서는 두진후안진의 방향에 따라 발생빈도에 유의한 차이를 보였으며, 주로 병변반대측으로 향하는 경우가 많았다(p<0.001) (Fig. 1).

Distribution of patients with pseudo-spontaneous nystagmus or head-shaking nystagmus in HC-BPPV. PSN beats more to the lesion side in apogeotropic HC-BPPV (*p=0.041), while geotropic subtype showed no directional preponderance of PSN (p=0.453). HSN beats more to the contra-lesion side in apogeotropic HC-BPPV (*p<0.001), while geotropic subtype showed no directional preponderance of HSN (p=0.136). HC-BPPV, horizontal canal benign paroxysmal positional vertigo; PSN, pseudo-spontaneous nystagmus; HSN, head-shaking nystagmus; Geo, geotropic subtype; Apo, apogeotropic subtype.
HC-BPPV 환자 197명 중 가성자발안진이 보이는 군(27명)과 가성자발안진이 보이지 않는 군(170명) 간의 임상적 특성을 비교해 보았을 때, 첫 치료 후 방문 시점 사이 간격의 평균 기간은 가성자발안진이 보이는 군은 2.7±2.2일(범위, 1–15일)이었고, 가성자발안진이 보이지 않는 군은 2.7±2.4일(범위, 1–9일)로 두 군 간 유의한 차이가 없었다. 또한, 연령 및 성별에는 유의한 차이를 보이지 않았으나, 어지럼의 발병부터 진단 시점까지의 기간은 가성자발안진이 보이는 군이 1.5±3.3일로 가성자발안진이 보이지 않는 군(3.8±7.8일)에 비해 유의하게 짧았으며(p=0.027), DHI점수는 가성자발안진이 보이는 군에서 63.0±16.0점으로 가성자발안진이 보이지 않는 군(38.9±24.6점)에 비해 유의하게 높은 점수를 보였다(p<0.001) (Table 2).
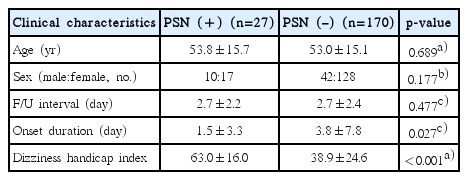
Comparison of clinical characteristics between PSN-positive and PSN-negative groups in horizontal canal benign paroxysmal positional vertigo
가성자발안진의 유무에 따라 BPPV의 치료 결과에 영향이 있을지 여부를 확인하였을 때, HC-BPPV 환자 전체 및 두 아형 각각에서 가성자발안진이 보이는 군과 보이지 않는 군 간에 치료 결과에는 통계적으로 유의한 차이를 보이지 않았다(Table 3).

Comparison of the number of canalith repositioning procedures required for the complete resolution between PSN-positive and PSN-negative groups in horizontal canal benign paroxysmal positional vertigo
고 찰
본 연구의 HC-BPPV 환자들에서 나타난 가성자발안진의 빈도는 13.7% (27/197명)이었으며, 두진후안진의 빈도는 45.2% (89/197명)이었다. 기존의 연구들에서 가성자발안진의 발생 빈도가 15%–76%, 두진후안진의 빈도가 30%–96%로 매우 다양하게 보고되고 있었으며[6-9], 본 연구의 결과는 기존 연구에서 보고된 빈도에 비해 상대적으로 낮은 빈도를 보였다. HC-BPPV에서 나타나는 가성자발안진 및 두진후안진에 대한 연구들이 매우 적었기 때문에 발생빈도의 범위도 다양하게 보고되고 있는 것으로 생각되며, 이렇게 다양한 결과들은 HC-BPPV 환자들이 진단되는 시점에서의 상태와 연관성이 있을 것으로 추정된다. HC-BPPV 환자들에서 이석의 움직임으로 팽대부마루가 휘어짐으로써 흥분성 신호가 발생한 상태에서 내원을 하게 되면 가성자발안진이 보이게 되는데[8,9], 환자들의 내원 및 진단 시점의 상태에 따라 가성자발안진의 빈도는 크게 차이가 나타날 수 있다. 그리고 가성자발안진의 유무는 체위 검사를 시행하기 전의 머리 위치에 따라 수평반고리관의 팽대부마루가 자극되었는지 여부와 연관성이 있으므로, 본 연구에 포함된 환자들은 기존 연구들에 비해 병원에 내원 시수평반고리관의 팽대부마루가 자극된 상태인 환자의 빈도가 적었을 것으로 추정된다.
본 연구에서 HC-BPPV 환자들에서 가성자발안진의 발생 빈도는 두 아형 간에 유의한 차이가 없었으나, 두진후안진의 발생 빈도는 HC-BPPV (Geo)보다 HC-BPPV (Apo)에서 더 흔하게 나타났다. HC-BPPV (Apo)에서 가성자발안진의 방향은 병변측으로 주로 나타났고, 두진후안진의 방향은 병변 반대측으로 주로 나타났다. 이러한 결과는 기존의 다른 연구들과 비슷한 결과를 보였다[8,9,11,12]. 본 연구의 HC-BPPV (Apo)에서 나타나는 가성자발안진의 방향이 병변측으로 주로 나타나는 것은 Fig. 2A에서와 같이 자발안진검사 시 앉은 자세일 때, 수평반고리관이 30° 정도 기울어져 있는 해부학적 구조 때문에 중력에 의해 팽대부마루에 이석이 붙음으로써 팽대부마루가 중력방향으로 휘어지기 때문으로 보인다[8,9,13]. 한 연구에 따르면 HC-BPPV 환자들의 가성자발안진의 방향이 앉은 자세에서 고개를 앞으로 숙일 때 반대 방향으로 바뀌게 되고, 고개를 뒤로 젖히면 다시 안진의 방향이 바뀌어 처음의 가성자발안진과 같은 방향으로 향하게 된다고 보고하였다[8]. 이렇게 HC-BPPV 환자들에서 끄덕평면에서의 머리의 움직임에 따라 가성자발안진의 방향이 바뀌는 것은 머리숙임-젖힘검사에서 발생하는 안진의 변화와 같은 원리로 설명할 수 있다.

Possible mechanism of PSN and HSN in apogeotropic horizontal canal benign paroxysmal positional vertigo. As a horizontal canal is bent 30° upward from the horizontal plane at rest in the sitting position, otoconia can slowly attach to the cupula by gravity and induce cupular deflection toward the utricular side, leading to PSN beating toward the ipsilesional side (A). After head-shaking, the impaction of otoconia near the inlet of the ampulla may result in endolymphatic flow blockage. The impaction of otoconia may prevent any cupular movement and result in asymmetric velocity storage, leading to HSN beating toward the contralesional side (B). PSN, pseudo-spontaneous nystagmus; HSN, head-shaking nystagmus.
본 연구의 HC-BPPV (Apo)에서 두진후안진의 방향이 병변 반대측으로 주로 나타나는 것은 다음과 같은 기전에 의한 것으로 추정해 볼 수 있다. Fig. 2B에서와 같이 HC-BPPV(Apo)에서는 병인이 되는 이석의 위치가 팽대부마루에 붙어 있거나 팽대부마루 근처에 있어 두진후안진검사 시 머리 회전에 의해 이석이 이동하여 좁아진 반고리관 부위에 기계적인 막힘이 일어나게 된다[8,9]. 그로 인해 병변측 수평반고리관 내림프액의 흐름이 방해되고 일측 전정기능의 장애가 유발되어 반대측 수평반고리관만 기능함으로써, 비대칭적인 속도저장기전(velocity storage mechanism)을 일으켜 병변 반대측으로 향하는 두진후안진을 유발한다[9,14,15]. 반면 HC-BPPV (Geo)에서는 두진후안진의 발생빈도가 흔하지 않고, 두진후안진의 방향우위도 특별히 없었다. 이에 대해 기존의 연구에서도 HC-BPPV (Geo)의 병태생리를 고려할 때 수평반고리관 내의 팽대입구부로부터 어느 정도 거리가 있는 곳에서 떠다니는 이석은 두진후안진검사 시 내림프액의 이동에 큰 영향을 미치지 않을 것으로 설명하고 있다[9].
가성자발안진의 유무에 따른 임상적 특성을 비교해 보았을 때, 가성자발안진이 보이는 그룹에서 어지럼의 발병부터 진단 시점까지의 기간은 1.5일로 가성자발안진이 보이지 않은 그룹의 3.8일에 비해 짧았으며, DHI점수는 평균 63.0점으로 가성자발안진이 보이지 않은 그룹의 38.9점보다 통계적으로 유의하게 높은 점수를 보였다. 이는 앞서 설명한 것처럼, HC-BPPV 환자들이 병원에 내원하여 진단하는 시점에 수평반고리관이 자극된 상태의 여부와 연관성이 있으며, 가성자발안진이 보이는 군의 환자들은 수평반고리관의 자극으로 인해 어지럼증 증상이 더 심한 상태이고, 그로 인해 병원에 내원하게 되는 기간이 짧았기 때문이라고 추정할 수 있다.
본 연구의 HC-BPPV 환자에서 자발안진의 유무에 따른 치료 결과에는 유의한 차이가 없었고 각 아형 내에서도 가성자발안진의 유무에 따른 치료 결과에는 차이가 없었다. 가성자발안진의 유무와 치료결과 간의 상관관계에 대한 기존의 연구는 거의 없었으며, 기존의 연구에서는 가성자발안진이 보이는 HC-BPPV 환자에서 치료 결과가 더 좋지 않고, 특히 HC-BPPV (Apo)에서 치료 결과가 더 좋지 않다고 보고하였다[16]. 하지만 기존의 연구에서는 모집단이 매우 적은 10명을 대상으로 분석하였으며, 상관관계에 대한 기전을 설명하지 않았다. 가성자발안진이 있는 경우 환자의 증상 및 강도가 심할 수 있으며 치료의 성공률이 떨어질 수 있다고 추정할 수 있으나, 본 연구의 결과에서는 큰 연관성을 찾을 수 없었다. 하지만 이 역시도 더 많은 대규모 환자에서의 연구가 시행되어야 좀 더 정확한 결론에 이를 수 있을 것으로 보인다.
본 연구가 후향적 연구라는 점과 기존의 가성자발안진이 나타나는 HC-BPPV 환자들에 대한 연구에서의 환자 표본 수보다는 많았지만, 아직 제한적인 환자 수 내에서의 연구였다는 점은 아쉬운 점이다.
HC-BPPV 환자에서 가성자발안진의 발생 빈도에는 아형 간에 유의한 차이를 보이지 않았으나 두진후안진의 발생빈도는 향지성 아형보다 원지성 아형에서 흔하게 발생하였다. 또한 HC-BPPV (Apo)에서 가성자발안진의 방향은 주로 병변측으로 향했고, 두진후안진의 방향은 주로 병변반대측으로 향했다. 본 연구를 통해, 가성자발안진이 보이는 HC-BPPV 환자들에서 어지럼증 증상의 정도가 더 심하고, 어지럼의 발병부터 BPPV의 진단까지의 기간이 짧다는 것을 알 수 있었다. 이 연구 결과는 가성자발안진이나 두진후안진이 보이는 HC-BPPV 환자들의 진단과 치료에 참고가 될 수 있을 것으로 기대된다.
Notes
No potential conflict of interest relevant to this article was reported.