코로나바이러스감염증-19 예방접종 후 전정신경염 1예
Vestibular Neuritis after COVID-19 Vaccination
Article information

Trans Abstract
Coronavirus disease 2019 (COVID-19) spread rapidly and was declared a pandemic. In this situation, vaccination for COVID-19 is important and has been prompted in many countries. However, a number of adverse events have been reported for the Pfizer, Moderna, and AstraZeneca vaccines. Otolaryngologic adverse events after COVID-19 vaccination were reported, including several cases of sudden sensorineural hearing loss. Vestibular neuritis (VN) is an acute vestibular syndrome that causes acute and spontaneous vertigo due to unilateral vestibular deafferentiation, leading to nausea or vomiting and unsteadiness that can last from days to weeks. Neurotropism for the cochleovestibular nerve, immunoglobulin G mediated immune off-target reaction, and reactivation of latent viruses are hypothesized to be etiologies. Herein, the case of a 49-year-old female who developed VN after COVID-19 vaccination is presented. Although the association between VN and COVID-19 vaccination remains unclear, clinicians should be aware that VN may occur as an adverse event of COVID-19 vaccination.
서 론
중증급성호흡기증후군 코로나바이러스 2 (severe acute respiratory syndrome coronavirus 2)로 인한 코로나바이러스 감염증-19 (coronavirus disease 2019, COVID-19)가 빠르게 확산하여 팬데믹이 선언되었고, 이러한 상황에서 COVID-19 예방접종은 전 세계적으로 중요하고 시급한 관심사이다[1]. 미국 식품의약국(U.S. Food and Drug Administration, FDA)은 2020년 12월 Pfizer-BioNTech 및 Moderna messenger RNA (mRNA) 기반 COVID-19 백신에 대한 긴급 사용 승인을, 2021년 2월 Janssen 재조합 아데노바이러스-벡터 COVID-19 백신에 대한 긴급 사용 승인을 발표했으며, Pfizer-BioNTech COVID-19 백신은 2021년 8월에 FDA의 완전한 승인을 받았다. 이후 많은 국가에서 COVID-19 백신 접종이 신속하게 진행되었다[2].
Janssen COVID-19 백신 접종 후 길랑-바레(Guillan-Barré)증후군 및 혈소판 감소 증후군을 동반한 혈전증, Pfizer-BioNTech 및 Moderna COVID-19 백신 접종 후 심근염을 포함하여 모든 심각한 부작용이 보고되었으며, 연관성은 아직 명확하지 않지만 COVID-19 예방접종 후 갑작스런 청력 상실도 보고되었다[2,3].
전정신경염(vestibular neuritis)은 편측성 전정신경쇠약으로 인한 급성 및 자발성 현기증을 유발하는 급성 전정증후군으로, 메스꺼움 또는 구토 및 불안정성이 수일에서 수주 지속된다[4]. 그동안 국내에서는 COVID-19 예방접종 후 전정신경염 발생 사례 1예가 보고된 바 있다[5]. 이에 저자들은 COVID-19 예방접종 후 전정신경염이 발병한 49세 여성의 사례를 보고한다.
증 례
49세 여자 환자가 2일 전에 발생한 급성 어지럼으로 외래를 방문하였다. 특이 과거력은 없었으나, 그녀는 현기증이 발병하기 6시간 전에 Pfizer-BioNTech 의 COVID-19 백신 1차를 맞았다. 동반되는 청력 저하의 증상은 없었고 최근 상부 호흡기 감염의 병력도 없었다. 또한 중추성 현기증을 의심하는 신경학적 징후나 증상은 없었으며, 내원 전 일 타 병원 응급실을 방문하였고, 이때 시행한 뇌 확산 강조영상(brain diffusion magnetic resonance imaging)과 뇌 컴퓨터 단층촬영(brain computed tomography)에서 중추성 병변을 포함한 특이 소견은 보이지 않았다. 이학적 검사에서 양쪽 고막은 정상이었고 우측 수평 자발성 안진이 관찰되었다. Dix-Hallpike 검사와 누워머리돌리기검사(supine roll test)에서 특징적인 회전성 또는 수평성 안진이 추가적으로 관찰되지 않았으며 우측 수평 자발성 안진만이 지속적으로 관찰되었다. 두진후안진 검사(head shaking test)에서 우측 수평 자발성 안진의 강화를 보였으며, 두부충동 검사(head impulse test)에서는 좌측의 교정신속보기(corrective saccades)가 관찰되었다. 환자는 심한 어지럼 증상으로 보존적 치료를 위해 입원하였다.
발병 3일 후 순음청력검사, 어음청력검사, 비디오 두부충동검사, 경부전정유발근전위를 시행하였다. 온도안진 검사(caloric test)는 환자의 어지럼이 심하여 시행 중 검사 거부로 시행하지 못하였다. 순음청력검사, 어음청력검사에서 청력은 정상 범위였으며 비디오 두부충동검사에서는 좌측 반고리관에서 추격 단속이 있으며 전정-안구 반사 이득의 감소가 관찰되었다(Fig. 1). 또한 경부전정유발근전위에서 좌측 전정유발근전위의 진폭 감소가 67%로 관찰되었다(Fig. 2). 이에 좌측 전정신경염이 진단되었다. 전정 억제제로 입원한 지 4일 후 현기증 증상이 개선되었고 자발적인 안진이 사라져 환자는 전정 재활에 대한 지시를 받은 후 퇴원하였다. 발병 10일 후 현기증 증상은 더욱 개선되었지만 경미한 증상이 남아 있었고, 지속적인 전정 재활을 교육하였다.
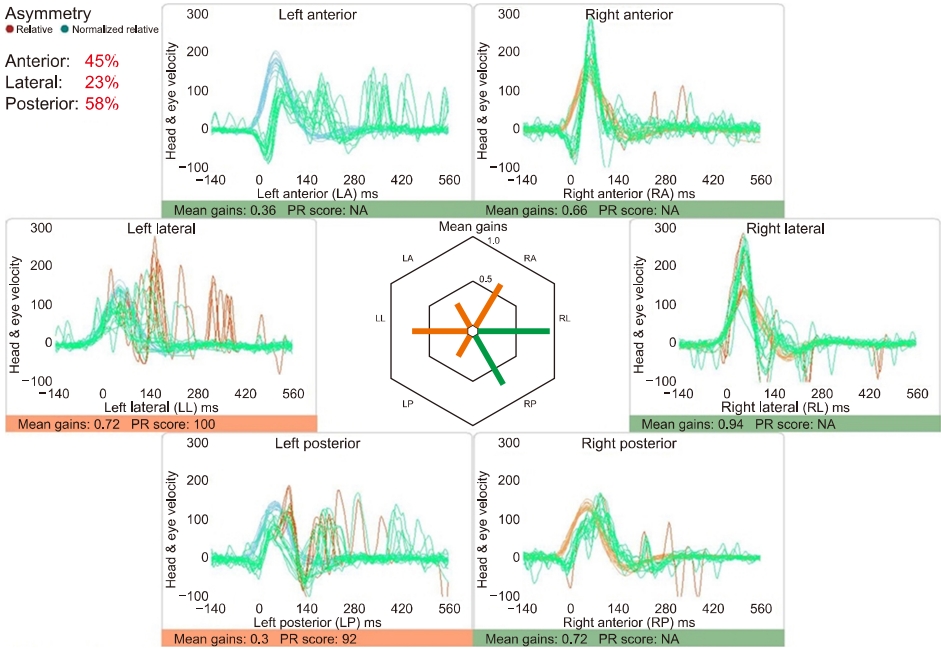
Three days after onset, there was a decrease in vestibulo-ocular reflex gain with catch-up saccade in the left anterior, lateral, posterior semicircular canal on video head impulse test. PR score, Perez and Rey score; NA, not available.
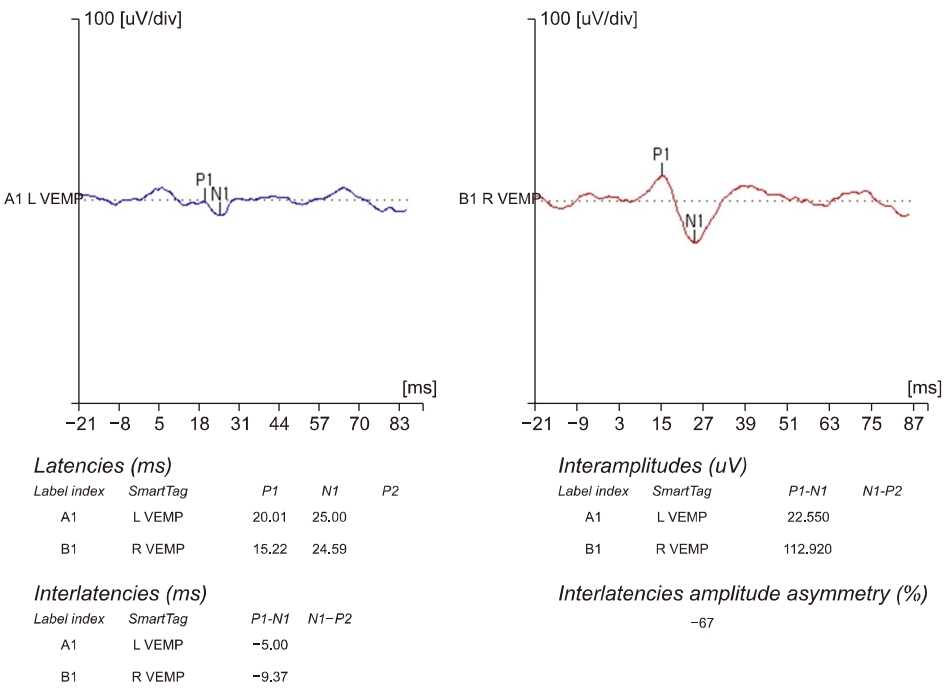
Three days after onset, the amplitude decrease of vestibular evoked myogenic potential was observed to be 67% on the left side. L, left; R, right; VEMP, vestibular evoked myogenic potential.
고 찰
전정신경염은 메스꺼움이나 구토를 동반한 갑작스러운 현기증, 불안정한 걸음걸이, 두위 변화에 따른 불균형, 수일에서 수주 동안 지속되는 자발적인 안진을 특징으로 하는 급성 전정 증후군이다[6]. 전정신경염은 청각 장애와 관련이 없으며 온도안진검사 또는 비디오 두부충동검사로 일측의 말초 전정 손상의 확인이 필요하다[7].
안면마비를 제외하고 이비인후과 증상과 COVID-19 mRNA 백신 사이에 가능한 인과 관계를 보고하는 증례 연구는 현재까지 거의 이뤄지지 않았다. 처음으로 보고된 연구는 Pfizer-BioNTech 백신 접종 직후 발생하는 이명에 대한 3건의 증례 보고였는데, 이 중 2건은 첫 접종 후 7–20시간 사이에 증상이 나타났고, 1건은 2차 접종 후 7일 사이에 증상이 나타났다[8]. 또한 최근 발표된 mRNA 백신 접종 후 이과적 안전성을 다루는 후향적 증례군 연구에서 30건의 청각 전정 증례가 확인되었다. 가장 흔한 증상인 청력 저하는 25명의 환자(83.3%)에서 보고되었으며, 이명 15명(50%), 현기증(dizziness) 8명(26.7%), 현훈(vertigo) 5명(16.7%)이었다. 증상 발현의 평균 시간은 백신 접종 후 10.18±9일이었고 범위는 1일에서 42일이었다[2]. 또 다른 증례군 연구에서는 Pfizer-BioNTech 백신(n=2) 및 Oxford-AstraZeneca 백신(n=1)으로 예방접종을 받은 세 명의 환자에서 청력 저하가 발생했다고 보고했다. 평균 발병 시간의 범위는 백신 접종 후 0–3일이었고 2건은 첫 번째 접종 후, 1건은 두 번째 접종 후 발생했다[9].
mRNA 백신과 관련된 이과적 질환에 대한 병태생리학적 기전에 대해 몇 가지 가설이 제기되고 있다. 첫째, 내이 또는 전정 와우 신경에 바이러스 침범으로 인한 와우염 또는 신경염으로 현훈, 이명 및 청력 저하가 유발될 수 있다[10]. 둘째, 자가반응성 T-림프구(autoreactive T-lymphocytes)와 관련된 자가면역 반응과 백신 항원이 분자적 모방을 통해 말초 면역 관용을 일시적으로 회피하여 전정 와우신경 또는 안면신경의 염증 반응을 유도할 수 있다[11]. 셋째, 예방접종 후 잠복 바이러스가 재활성화되어 전정신경염을 유발할 수 있다[2,12]. 넷째, 와우 모세관의 국소 손상과 같은 내피 장애 또는 예방접종에 대한 불안함이 mRNA 백신과 관련된 이명의 원인으로 가정되었다[8]. 마지막으로, 백신 접종 후 증상 발병까지의 시간이 평균 10일로 관찰되는 증례에서 전정 와우신경에 대한 immunoglobulin G 매개 면역 오프타겟 반응(off-target reaction)이 가능한 기전이 될 수 있다[2]. 그러나 이 가설은 첫 번째 접종을 받고 이전 COVID-19 감염이 없는 환자에서 예방 접종 직후 증상이 발생하는 경우를 설명하지 못한다.
전정신경염의 치료에는 급성기의 전정 억제제를 사용한 증상 치료와 지속적인 전정 재활이 포함된다[4,13]. 코티코스테로이드(corticosteroid)의 효능은 여전히 논란의 여지가 있다[4]. 그러나 심한 경우에는 코티코스테로이드를 사용할 수 있다[13]. 다만, 예방접종 후 전신 스테로이드의 효과는 조사되지 않았다. 따라서 즉각적인 전신 스테로이드 사용은 백신 접종에 대한 항체 형성에 영향을 줄 수 있으므로 백신 접종 후 스테로이드 사용에 주의해야 한다.
이 경우 전정신경염은 COVID-19 백신 접종 후 1일 이내에 발생했다. 그 동안의 다른 연구들을 살펴보았을 때, COVID-19 판데믹 이전과 비교하여 전정신경염 발병률에 통계적으로 유의한 증가는 관찰되지 않아, 전정신경염과 COVID-19 예방접종 간의 시간적인 근접성 이외에 연관성은 아직 명확하게 밝혀진 바는 없다[14]. 하지만, 백신의 안전성을 지속적으로 평가하여 예방접종 인구에 대한 위험을 최소화하기 위하여 임상의는 전정신경염이 COVID-19 예방접종의 부작용으로 발생할 수 있음을 알고 있어야 한다.
Notes
이해관계(CONFLICT OF INTEREST)
저자들은 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.
연구 지원(FUNDING/SUPPORT)
본 연구는 2022년도 가톨릭대학교 부천성모병원 임상 연구비 지원을 받아 수행되었습니다.
저자 기여(AUTHOR CONTRIBUTIONS)
Conceptualization: SHK, SHH; Data curation: SHK; Formal analysis: SHK; Funding acquisition: SHH; Investigation: SHH; Methodology: SHK, SHH; Project administration: SHK, SHH; Visualization: SHK, SHH; Writing–original draft: SHK, SHH; Writing–review & editing: SHK, SHH.
All authors read and approved the final manuscript.