Abstract
- Ramsay Hunt syndrome occurs when the varicella zoster virus reactivates. Classic findings include the triad of facial paralysis, otic pain and herpetic lesions due to the pathogenesis associated with anterograde axonal reactivation of the varicella zoster virus in the geniculate ganglion. In addition to the classic triad, rare features such as a central type of vestibular function test may be observed due to the retrograde spread of the varicella zoster virus from the geniculate ganglion into the brain stem, including involvement of the vestibular nucleus. We present a case of Ramsay Hunt syndrome in a 57-year-old male patients, manifesting not only the typical triad of symptoms but also the unique features associated with brain stem involvement. This presented as direction-changing gaze-evoked nystagmus and a decrease in gain on both sides on video head impulse test. And brain magnetic resonance imaging showed a lesion in the vestibular nucleus of the brain stem.
-
Keywords: Ramsay Hunt syndrome; Herpes zoster oticus; Brain stem
-
중심단어: 람세이-헌트 증후군, 이성대상포진, 뇌간
서 론
람세이 헌트 증후군(Ramsay Hunt syndrome)은 대상포진 바이러스(varicella zoster virus, VZV)에 의해 발병하는 질환으로 급성 말초성 안면마비, 이개 및 안면부의 대상성 포진 등의 증상을 동반하며, 주로 VII, VIII번 뇌신경을 침범하지만 드물게는 III, IV, V, VI, IX, X, XI, XII번 뇌신경의 마비도 동반하여 안구운동 장애, 안면부 감각이상, 애성, 연하곤란, 흉쇄유돌근의 위축, 혀 운동 장애 등의 다발성 뇌신경 마비 증상도 나타날 수 있다[1,2]. 람세이 헌트 증후군은 안면신경의 슬신경절(geniculate ganglion)에 잠복해 있던 VZV가 재활성화하여 발생하는 것으로 알려져 있으며[3], 드물지만 다발성 뇌신경 마비 및 중추신경계 침범도 가능하다. 이에 대해서는 바이러스가 축삭(axon)을 통한 역행성(retrograde) 전파로 직접적으로 뇌간과 같은 중추계 실질에 침범한다는 가설과, 바이러스로 인한 혈관병증(vasculopathy)으로 인해 뇌간(brain stem) 및 여러 뇌신경을 공급하는 혈관에서 허혈성 경색 및 출혈이 발생하여 다발성 뇌신경 마비 및 중추신경계 침범이 발생한다는 가설이 있다[4].
저자들은 어지럼증, 청력 저하 및 우측 이개 통증을 주소로 내원하여 람세이 헌트 증후군으로 진단받은 환자의 경과 관찰 중 증상 발생 17일째 우측 안면마비 소견이 관찰되었고, 비디오 안진검사(videonystagmography)에서 방향 전환성 주시유발안진(direction-changing gaze-evoked nystagmus) 소견 및 비디오 두부충동검사(video head impulse test)상 양측에서 이득(gain)이 감소한 소견이 보였으며, 뇌 자기공명영상에서 뇌간의 전정 핵(vestibular nucleus) 주변에서 고신호를 보이는 병변을 확인했다. 이에 뇌간 침범을 동반한 람세이 헌트 증후군을 치료한 경험을 공유하여 임상적인 도움을 주고자 한다.
증 례
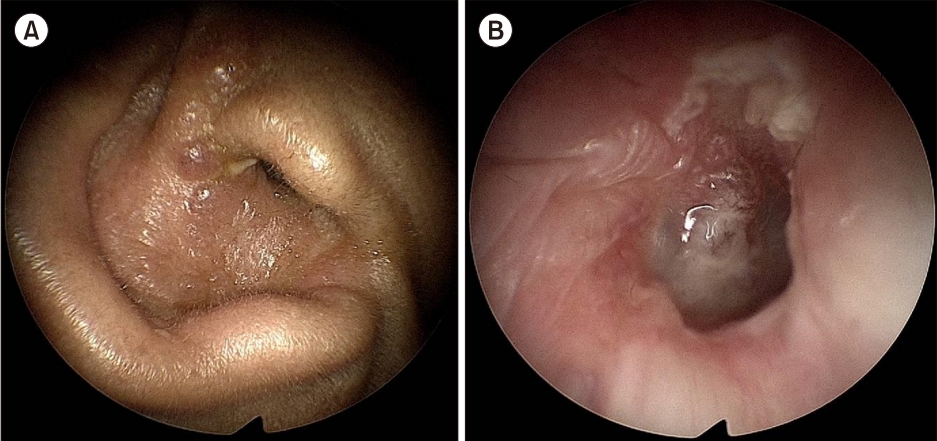
57세 남자 환자가 4일 전부터 발생한 우측 이개 통증 및 수포를 주소로 본원 응급실로 내원하였다. 과거력 및 가족력에 특이사항은 없었고, 청력 저하, 어지럼증, 안면마비 증상은 호소하지 않았다. 이학적 검사에서 우측 이개에 국한된 수포성 병변, 외이도 및 고막의 발적과 삼출액이 관찰되었고(Fig. 1), 자발안진(spontaneous nystagmus)은 관찰되지 않았다. 환자는 발병 5일째 우측 청력 저하 및 자세변화와 관계없이 지속되는 불균형(disequilibrium) 양상의 비회전성 어지럼증을 호소하였고, 발병 7일째 시행한 순음청력검사에서 우측 기도 68 dB, 골도 58 dB의 혼합성 난청을 보였다. 어음청력검사에서 우측 60%의 어음명료도를 보였고, 좌측은 기도 15 dB, 골도 11 dB, 어음명료도 100%로 정상이었다. 비디오 안진검사에서는 좌측으로 향하는 수평 자발안진이 관찰되었고, 좌측 주시 시 안진의 완서상 속도가 증가하는 Alexander 법칙을 따랐으며, 우측 주시 및 시 고정에는 안진이 억제되었다(Fig. 2A). 냉온교대 온도안진검사에서 우측 100%의 반고리관 마비 소견이 보였고, 비디오 두부충동검사에서 우측 세 반고리관에서 이득 감소를 보였다(Fig. 3A). 이학적 검사에서 우측 안면마비 소견은 관찰되지 않았다. 이에 경구용 스테로이드(prednisolone, 60 mg/일)를 6일간 사용 후 4일에 걸쳐 용량을 감량하였고, 항바이러스제(famciclovir, 750 mg/일)를 1주간 사용하였다.
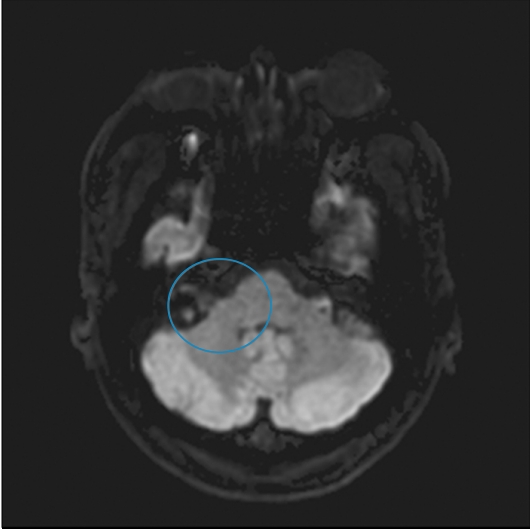
환자는 발병 17일째 우측 이개 통증 및 수포성 병변은 호전 추세였고 불균형 양상의 어지럼증은 호전을 보이다가 다시 악화되었으며, 우측 안면마비 증상이 처음으로 동반되어 응급실에 재내원하였다. 당시 시행한 이학적 검사에서 우측 이개의 수포성 병변 및 외이도, 고막의 발적은 대부분 호전된 상태였으며, 우측 안면마비는 하우스-브랙만 등급(House-Brackmann grade) 3등급이었다. 응급실에서 시행한 Frenzel 안진검사에서 우측으로 향하는 수평 자발안진이 관찰되었고, 우측 주시 시에 안진의 강도가 증가하였다. 두부충동검사에서 머리를 우측으로 회전할 때 양성이었으나 좌측으로 회전 시에는 음성이었다. 그 외 다른 신경학적 증상은 동반되지 않았으며, 뇌 확산 강조 자기공명영상에서 급성 중추성 병변은 관찰되지 않았다(Fig. 4).
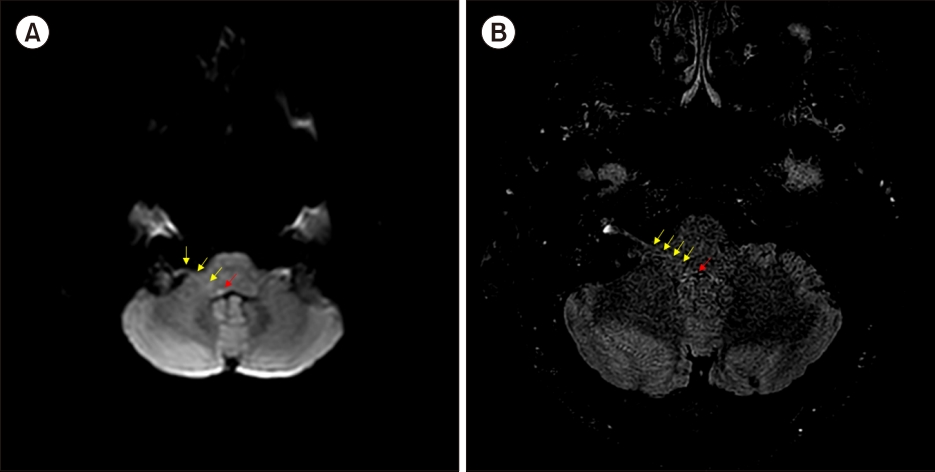
발병 20일째 외래로 내원하여 시행한 비디오 안진검사에서 좌측으로 향하는 수평 자발안진이 관찰되었고, 좌측 주시 시 좌측으로 향하는 안진이 관찰되었으나 우측 주시 시에 우측으로 향하는 안진이 관찰되는 방향 전환성 주시 유발안진 소견을 보였다(Fig. 2B). 비디오 두부충동검사에서는 양측 후반고리관, 측반고리관에서 이득이 감소하였다(Fig. 3B). 우측 안면마비 및 청력의 호전은 없었다. 그 외 수직 방향의 스큐 편위 및 다른 신경학적 증상은 관찰되지 않았으나, 환자의 어지럼증이 악화하였고 HINTS 검사(head impulse test, direction-changing gaze-evoked nystagmus, test of skew)에서 방향 전환성 주시유발안진 양성 및 비디오 두부충동검사에서 양측 이득의 감소를 보였기에 전하소뇌동맥(anterior inferior cerebellar artery) 경색 등의 중추성 병변에 대한 평가 및 보존적 치료를 위해 입원하였다. 발병 23일째(입원 2일째)에 비디오 안진검사를 반복 시행하였고 방향 전환성 주시유발안진은 이전과 변화 없이 관찰되었으며, 신경전도검사(electroneuronography)에서 우측 눈둘레근(orbicularis oculi muscle)의 진폭(peak-to-peak amplitude)은 건측의 85.8%, 소근(risorius muscle)은 건측의 73.2%로 감소된 양상을 보였다. 뇌 자기공명영상에서 우측 상부 연수(medulla oblongata)의 등가쪽(dorsolateral)에서 고신호강도를 확인할 수 있었고, 다음날 반복 시행한 뇌 자기공명영상에서도 같은 부위에서 이전보다 신호가 증가된 소견을 보였다(Fig. 5). 환자는 청력 저하, 안면마비, 어지럼증 외에 복시, 연하장애, 사지의 감각장애, 구음 장애 등의 추가적인 신경학적 증상은 없었으며, VZV의 뇌간 침범을 고려하여 입원 중 스테로이드제(dexamethasone disodium phosphate, 10 mg/일)을 7일간 투여 후 3일간 용량을 감량하였고 항바이러스제(famciclovir, 750 mg/일)를 7일간 재복용하였다. 발병 60일째 외래 추적관찰 중 시행한 순음청력검사에서 우측 기도 62 dB, 골도 60 dB의 감각신경성난청 소견, 어음청력검사에서 우측 60%의 어음명료도를 보여 호전은 없었다. 비디오 안진검사에서는 좌측으로 향하는 수평 자발안진을 보였으나 시고정 시 억제되었으며, 좌측 주시 시 좌측으로 향하는 안진이 강화되었으나, 우측 주시 시에 안진은 관찰되지 않아 방향 전환성 주시유발안진은 더 이상 관찰되지 않았다. 비디오 두부충동검사에서는 우측 세 반고리관에서 이득이 감소하였고, 좌측은 측반고리관에서 이득 감소 소견을 보였다. 어지럼증은 더 이상 호소하지 않았으며, 우측 안면마비는 하우스-브랙만 1등급으로 호전되었다. 그 외 다른 신경학적 증상은 호소하지 않았다.
고 찰
VZV가 중추신경계를 침범하는 기전에 대해서는 여러 가지 가설이 존재한다. 첫 번째 가설은 VZV가 슬신경절로부터 신경의 축삭을 경유하여 역행성 전파를 통해 혈관 침범 없이 뇌간과 같은 중추신경계를 침범한다는 것이고[5], 두 번째 가설은 VZV가 뇌신경의 구심성(afferent) 섬유신경으로부터 신경 연접을 경유하여 뇌간으로 공급되는 혈관 구조를 침범하여 혈관병증을 일으켜 중추계의 허혈성 경색, 동맥류, 지주막하 출혈, 혈관 협착을 일으킬 수 있다는 것이다[4].
본 증례의 환자는 경구용 스테로이드(prednisolone, 60 mg/일)와 항바이러스제(famciclovir, 750 mg/일) 사용에도 불구하고 발병 17일째 우측 안면마비, 어지럼 악화 증세를 보였고, 뇌 자기공명영상의 확산텐서영상(diffusion tensor image)에서 연수의 우측 상부의 등가 쪽에서 신호 증가 소견이 관찰되었다. 이런 허혈성 병변의 원인들로는 VZV 감염의 중추신경계 침범으로 인해 발생했을 가능성과 VZV 감염과 별개로 환자의 신체적 상태로 인해 허혈성 병변이 발생했을 가능성 모두를 시사할 수 있으나, 환자의 연령이 젊고 특이 기저질환이 없음을 고려하였을 때 VZV 감염에 의해 뇌간의 허혈성 병변이 발생했을 가능성이 더 높다고 할 수 있다. 그리고 fluid attenuation inversion recovery (FLAIR) image에서 우측 안면 신경의 슬신경절, 이공분절(meatal segment), 두개내분절(intracranial segment) 줄기를 따라 FLAIR 신호 증가 소견을 보이는 것은 VZV가 안면 신경을 따라 역행성으로 전파되어 두개 내로 직접 감염된 병변으로 설명할 수 있다[6].
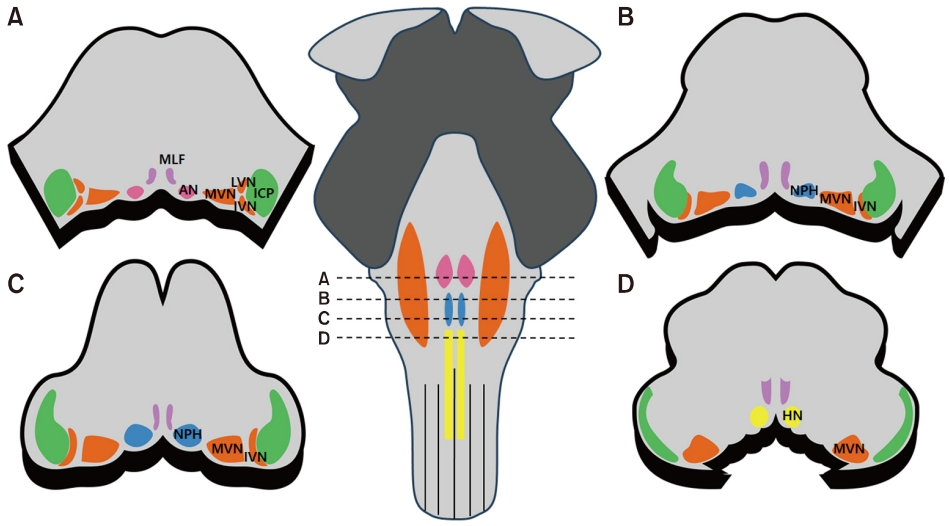
전정신경핵은 교뇌의 꼬리 부분에서 연수의 입 쪽까지 걸쳐 있으며, 4번째 뇌실(ventricle)의 바닥을 따라 뇌간의 등가 쪽에 양측으로 위치해 있다. 이는 외측전정핵, 내측 전정핵, 상전정핵, 하전정핵의 4개 주요 핵으로 세분화되며, 말초 전정신경섬유의 기착지로 전정 정보를 처리하는 중추 전정신경계 구조물이다. 이 중 내측전정핵은 4개 주요 핵 중 가장 내측에 위치하고, 가장 큰 부피를 차지하며 상전정핵과 함께 전정안구반사(vestibuloocular reflex)를 매개하는 역할을 한다[7]. 따라서 전정신경핵을 포함하는 병변은 말초 및 중추성 전정기능 장애 징후를 모두 나타낼 수 있다. 이 중 한 쪽의 내측전정핵 부위의 국소 병변은 비디오 두부충동검사에서 병변 쪽뿐만 아니라 병변 반대쪽에서도 측반고리관, 후반고리관 이득 감소를 보이는 데, 이는 전정신경핵 사이에 존재하는 건측으로의 억제성 사이신경원(interneuron)도 기능이 저하되어 이에 대한 적응기제로 인해 발생한 것으로 추정되고 있다[8]. 또한 내측전정핵 및 설하전 신경핵(nucleus prepositus hypoglossi)은 수평면의 신경 적분체(neural integrator) 기능을 담당하며 이를 통해 안구가 가측을 주시할 때 중심으로 끌려가지 않고 시선(gaze)을 목표점에 유지할 수 있게 하는 역할을 한다[9,10]. 따라서 신경 적분체를 포함하는 내측전정핵 또는 설하전 신경핵에 병변이 발생하게 되면 방향 전환성 주시유발안진과 같은 중추성 전정 이상이 발생하게 된다[10]. 환자의 비디오 안진검사에서 방향 전환성 주시유발안진 소견을 보이고 비디오 두부충동검사에서 양측의 이득이 감소한 소견을 보인 것은 상부 연수의 등가 쪽에서 보인 허혈성 병변이 내측전정핵 부위와 인접하여 발생한 것으로 추정할 수 있다(Fig. 6). 본원 영상의학과와 상의한 결과 환자의 뇌 자기공명영상에서 보인 병변의 위치는 Fig. 6B에 보이는 내측전정핵 부위와 일치할 것으로 생각된다는 의견을 얻었다. 발병 17일째 응급실에서 시행한 Frenzel 안진검사에서 건측으로 향했던 자발안진의 방향이 병변 측으로 바뀐 것은, 발병 초기에 관찰됐던 마비성(paralytic) 자발안진 이 중추 신경계 보상을 거쳐 회복 단계(recovery phase)에 진입하면서 보인 회복(recovery) 자발 안진이라고 볼 수 있다. 일측성 전정 이상으로 인해 중추신경계 보상 기전이 활성화되면 양측 정전 신경핵의 신경 활동 수준이 모두 감소되는데, 이를 통해 양측 말초성 말단 전정기관 사이의 신경 비대칭이 감소하게 된다. 이 단계의 보상 과정에서 손상된 쪽의 기능이 회복되면 병변측 귀의 긴장성 신경 출력(tonic neural activity)이 높아지면서 병변 측으로 회복 자발안진을 생성하게 되는데, 문헌에 따르면 회복 안진은 평균적으로 어지럼증 발생 후 17일 후에 발생한다고 한다[11,12].
HINTS 양성과 같은 중추성 전정 이상은 전하소뇌동맥의 경색에 의해서도 드물게 발생할 수 있으며, 이는 전하소뇌동맥이 소뇌 반구의 일부와 편엽(flocculus), 중소뇌각(middle cerebellar peduncle), 하뇌교(lower pons)의 V, VII번 뇌신경 핵, 와우 핵(cochlear nucleus) 및 VII, VIII번 뇌신경 뿐만 아니라 상전정핵 및 내측전정핵의 혈액 공급을 담당하기 때문이다[13,14]. HINTS는 head impulse test, directionchanging gaze-evoked nystagmus, test of skew의 약자로, 세 가지 중 하나만 해당되어도 중추성 현훈을 의심해야 하며, 발병 초기에 중추성 병변을 감별할 때 뇌 자기공명영상보다 더 효과적인 것으로 알려져 있다[15]. 본 증례의 경우 환자가 발병 17일째 안면마비와 함께 어지럼증 악화 소견을 보이면서 HINTS 양성 소견 및 두부충동검사에서 양측의 이득 감소 소견을 보였기에 전하소뇌동맥 경색과 같은 중추성 병변에 대한 감별이 우선적으로 필요하였고, 이에 시행한 뇌 자기공명영상에서 우측 연수 상부의 등가 쪽 부위와 전정와우신경의 줄기를 따라 병변이 관찰되었다. 본 증례는 이러한 병변의 원인을 정확히 추정하기 위해 혈관조영술, 뇌척수액검사 등을 시행하지 않았다는 제한점이 있으나, 환자는 람세이 헌트 증후군의 전형적인 증상을 보이는 중에 안면마비 발생과 함께 어지럼증 악화 소견을 보였고, 자기공명영상에서 이전 영상에서는 보이지 않았던 전정핵에 국한된 허혈성 병변이 확인된 점으로 보아 VZV 감염으로 인해 뇌간의 허헐성 병변이 발생했을 것이라고 추정할 수 있다.
람세이 헌트 증후군의 중추신경계 침범은 드물며, 면역력이 저하된 고령의 환자에서 발생한 경우가 대부분이었다. 본 증례는 특이 기저질환이 없는 비교적 젊은 환자에게 스테로이드 및 항바이러스제와 같은 적절한 치료를 시행하여도 뇌간 침범과 같은 중추성 병변으로 발전할 수 있음을 시사하며, 검사 시 HINTS 양성 소견과 같은 중추성 병변을 의미하는 결과가 나타날 수 있음을 보여주고 있다.
ARTICLE INFORMATION
-
이해관계(CONFLICT OF INTEREST)
저자들은 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.
-
연구 지원(FUNDING/SUPPORT)
해당 없음.
-
저자 기여(AUTHOR CONTRIBUTIONS)
Conceptualization: All authors; Data curation, Formal analysis, Investigation, Methodology, Visualization: MHL; Project administration: MBK; Writing–original draft: MHL; Writing–review & editing: All authors.
All authors read and approved the final manuscript.
Fig. 1.(A, B) Endoscopic examination of the right ear showed multiple vascular lesions on the auricle, along with inflammation and discharge in the external auditory canal and tympanic membrane.
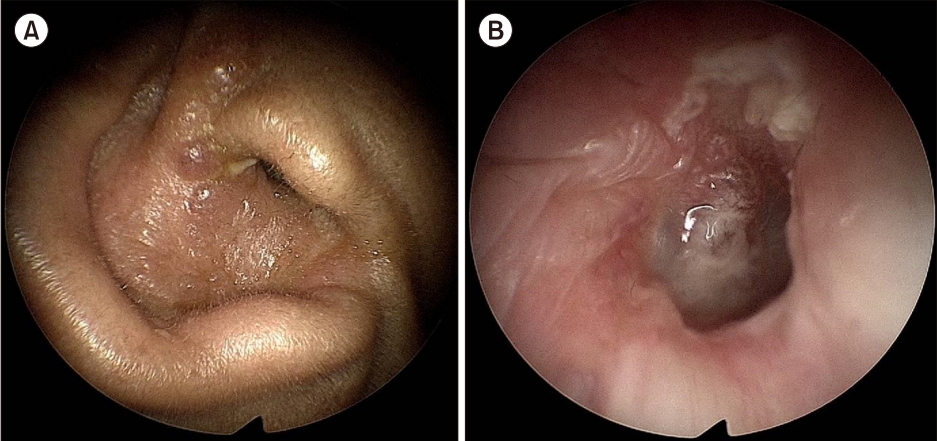
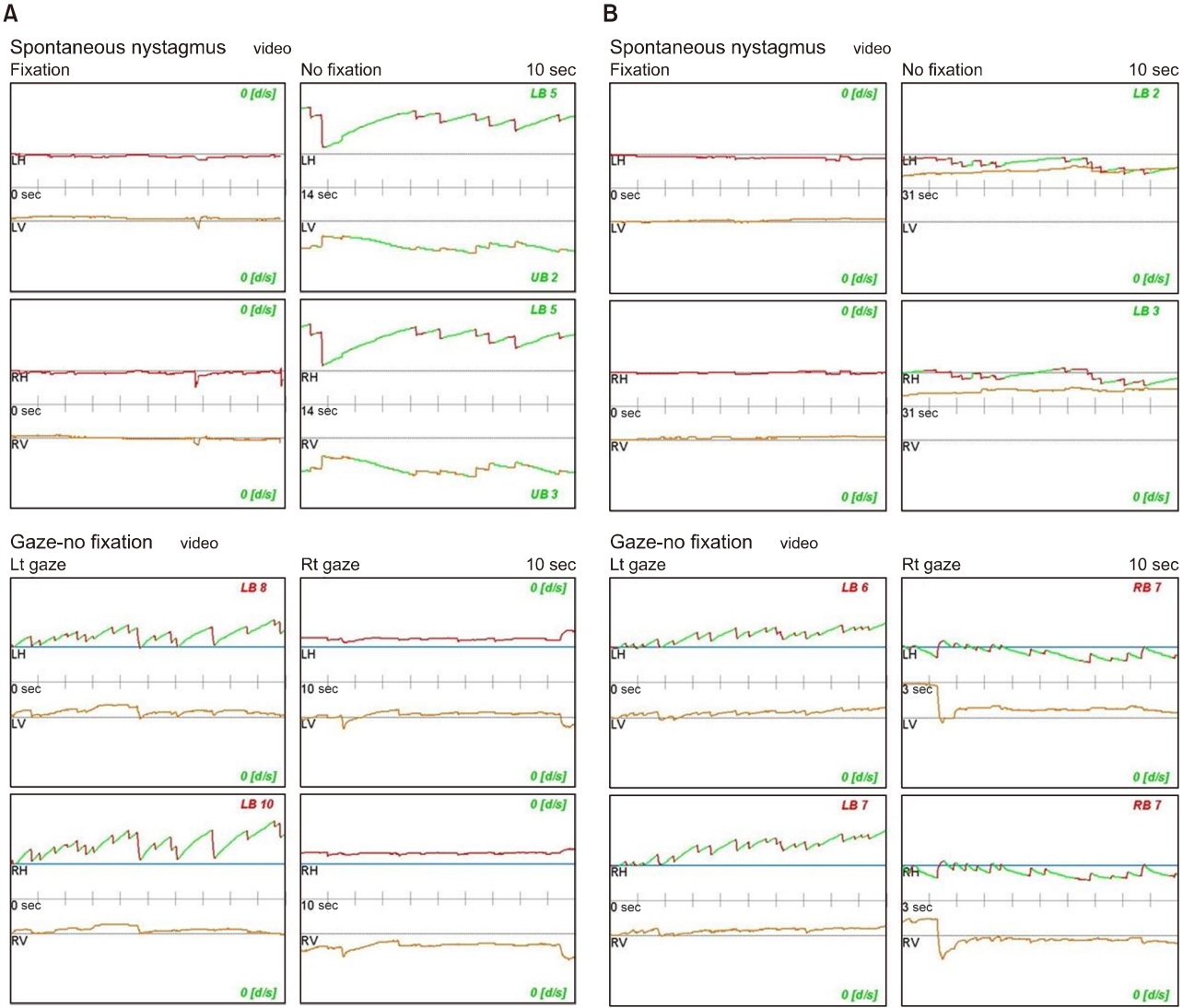
Fig. 2.(A) On the 7th day after the onset, videonystagmography showed findings suggestive of peripheral nystagmus, along with left-beating horizontal spontaneous nystagmus. (B) On the 20th day after the onset, videonystagmography showed left-beating horizontal spontaneous nystagmus. However, during right gaze-evoked nystagmus, right-beating horizontal spontaneous nystagmus was observed, indicating a central nystagmus pattern. LH, left horizontal; LV, left vertical; LB, left beating; RH, right horizontal; RV, right vertical; RB, right beating.
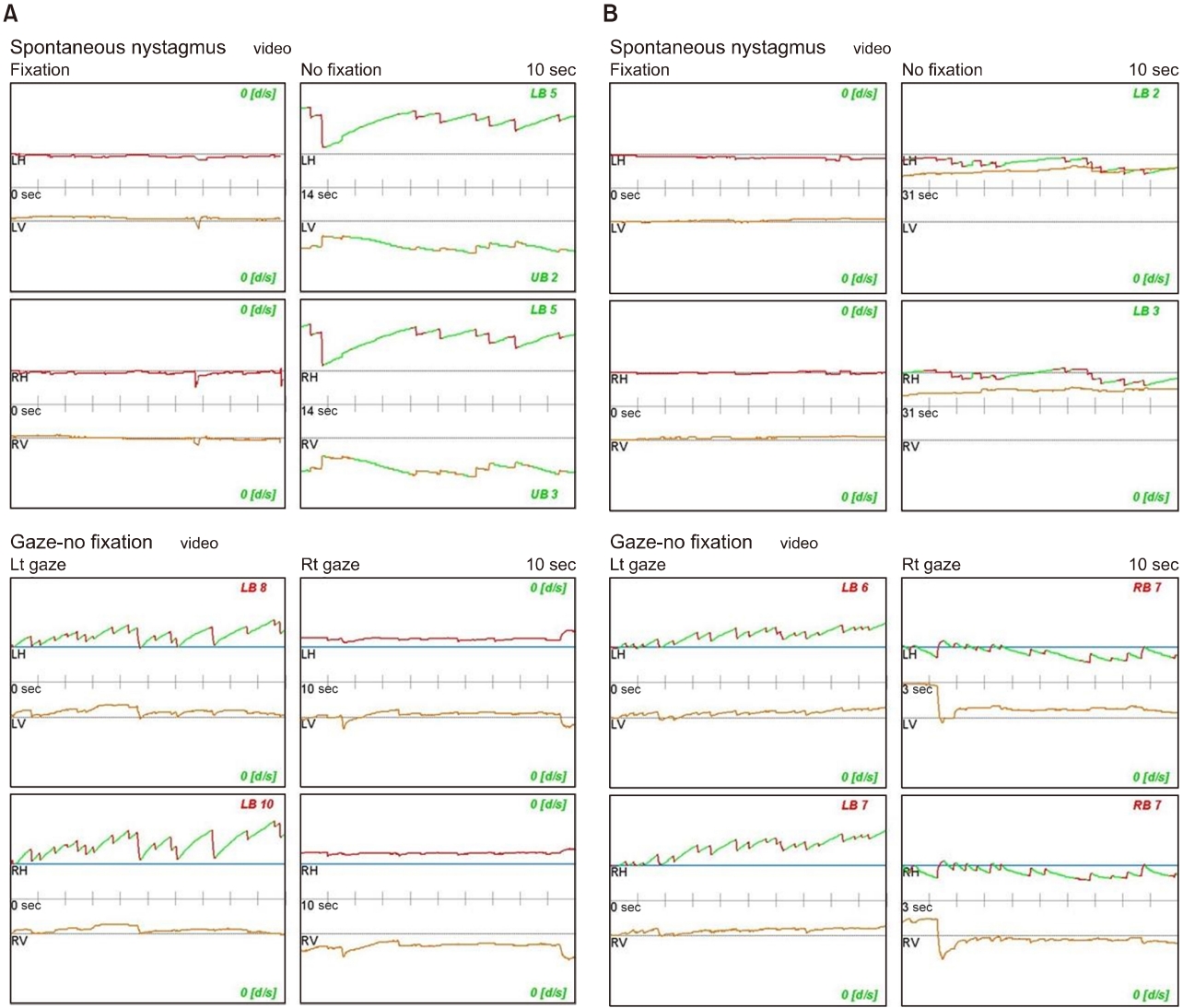
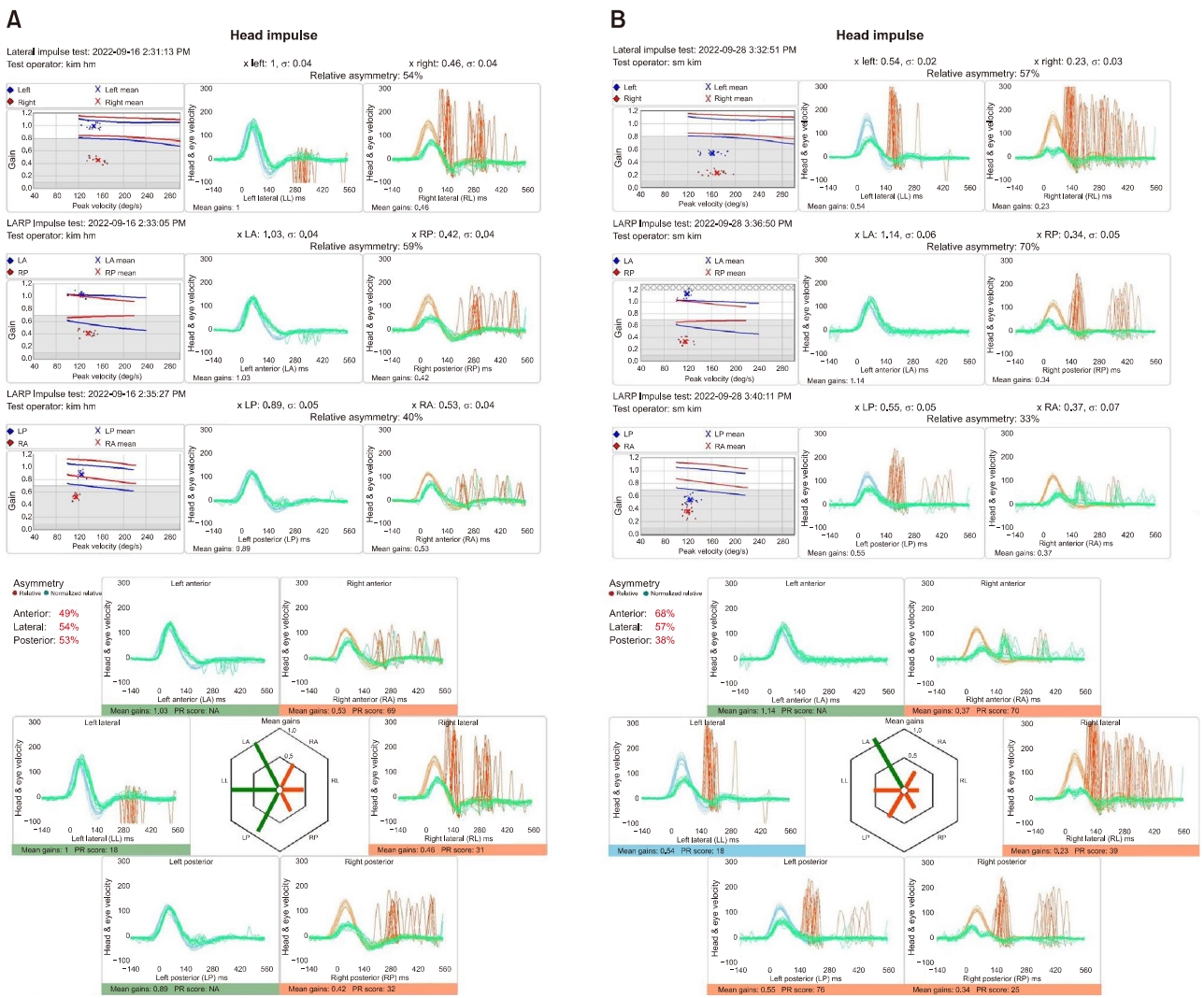
Fig. 3.(A) On the 7th day after the onset, video head impulse test (vHIT) showed catch-up saccades and reduced gain in the right lateral, posterior, and anterior semicircular canals. (B) On the 20th day after the onset, vHIT showed catch-up saccades and reduced gain in both the lateral and posterior semicircular canals, and reduced gain was also observed in the right anterior semicircular canal. LL, left lateral; LA, left anterior; LP, left posterior; RL, right lateral; RA, right anterior; RP, right posterior; PR score (coefficient of variance); NA, non available.
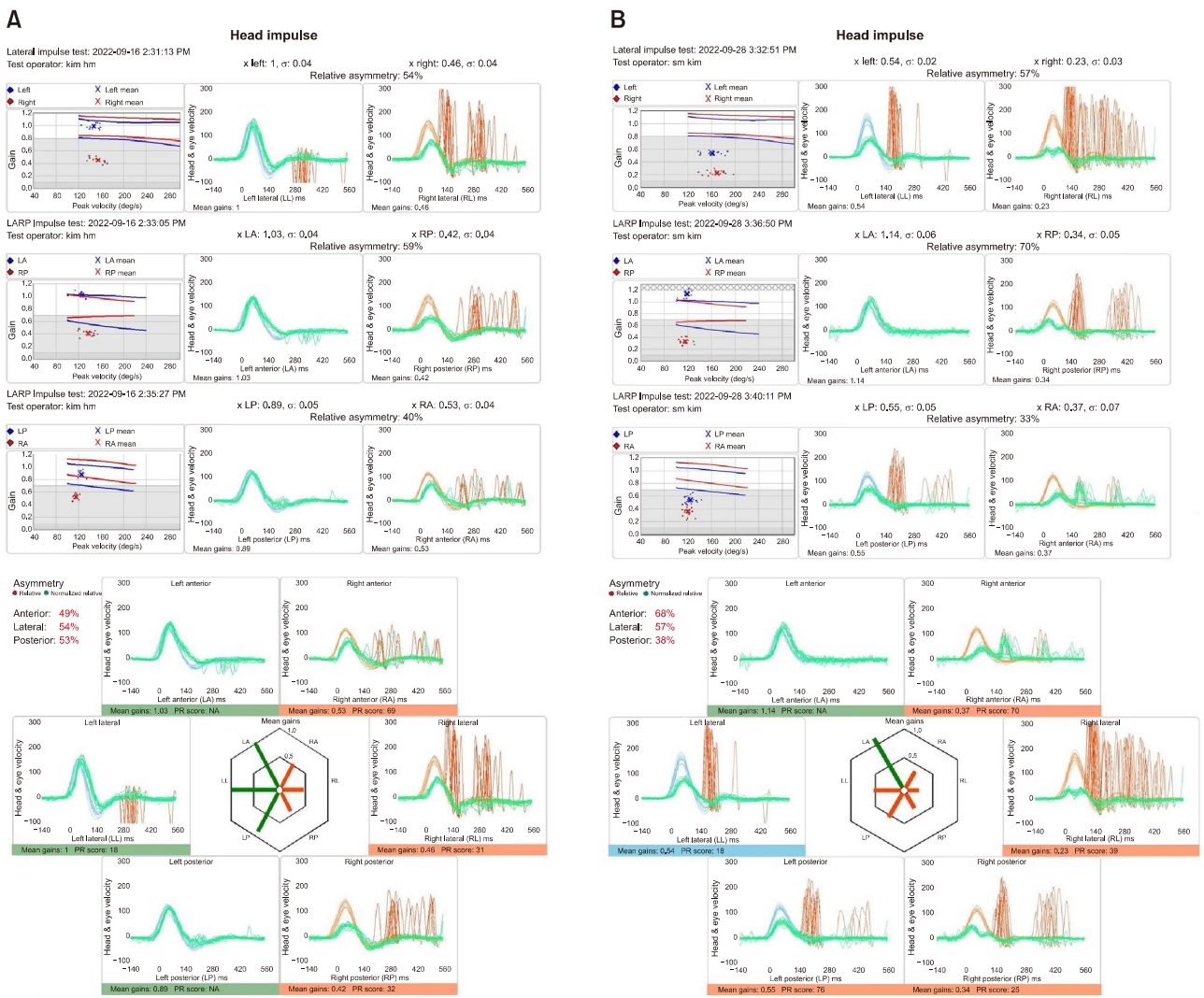
Fig. 4.Brain diffusion weighted image performed on the 17th day after the onset showed no evidence of acute central lesions (circle)
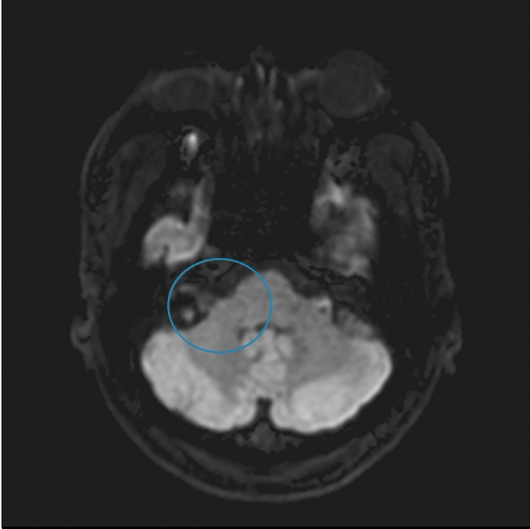
Fig. 5.Diffusion tensor image (A) and fluid attenuation inversion recovery image (B) performed on the 23rd day after the onset showed hyperintense signal in the right vestibular nucleus mainly (red arrows) and hyperintense signal in the section of upper medulla and cisterns of the facial nerve (yellow arrows).
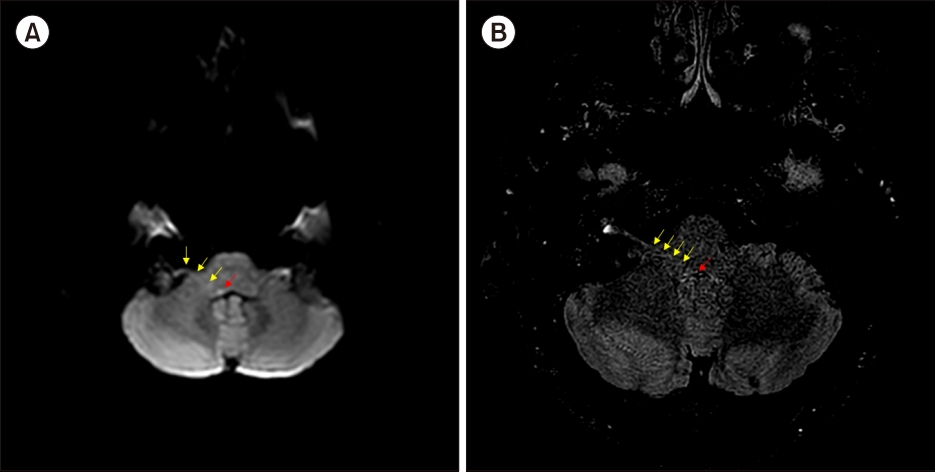
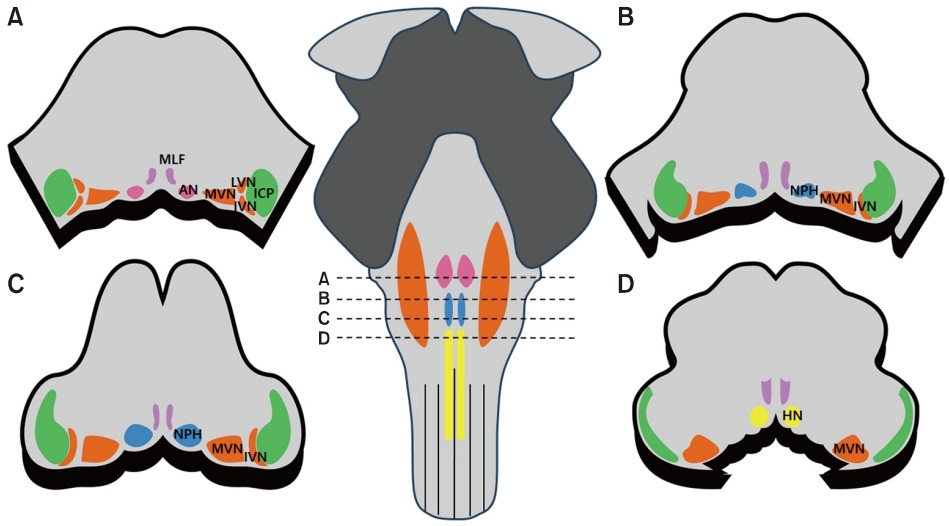
Fig. 6.Cross section of the brain stem. MLF, medial longitudinal fasciculus; AN, abducens nucleus; MVN, medial vestibular nucleus; LVN, lateral vestibular nucleus; ICP, inferior cerebellar peduncle; IVN, inferior vestibular nucleus; NPH, nucleus prepositus hypoglossi; HN, hypoglossal nucleus.
REFERENCES
- 1. Hunt JR. On herpetic inflammations of the geniculate ganglion. A new syndrome and its complications. J Nerv Ment Dis 1907;34:73–96.Article
- 2. Morelli N, Mancuso M, Cafforio G, Gallerini S, Pittiglio L, Tonelli S, et al. Ramsay-Hunt syndrome complicated by unilateral multiple cranial nerve palsies. Neurol Sci 2008;29:497–8.ArticlePubMedPDF
- 3. Kim KM, Yu K, Jeon EJ, Lee HJ. Herpes zoster oticus with delayed facial palsy and multiple cranial nerve involvement. Korean J Otorhinolaryngol-Head Neck Surg 2021;64:839–43.ArticlePDF
- 4. Gilden D, Cohrs RJ, Mahalingam R, Nagel MA. Varicella zoster virus vasculopathies: diverse clinical manifestations, laboratory features, pathogenesis, and treatment. Lancet Neurol 2009;8:731–40.ArticlePubMedPMC
- 5. Hu S, Walker M, Czartoski T, Cheng A, Forghani B, Gilden DH, et al. Acyclovir responsive brain stem disease after the Ramsay Hunt syndrome. J Neurol Sci 2004;217:111–3.ArticlePubMed
- 6. Bertrand A, Leclercq D, Martinez-Almoyna L, Girard N, Stahl JP, De-Broucker T. MR imaging of adult acute infectious encephalitis. Med Mal Infect 2017;47:195–205.ArticlePubMed
- 7. Khan S, Chang R. Anatomy of the vestibular system: a review. NeuroRehabilitation 2013;32:437–43.ArticlePubMed
- 8. Park HK, Kim JS, Strupp M, Zee DS. Isolated floccular infarction: impaired vestibular responses to horizontal head impulse. J Neurol 2013;260:1576–82.ArticlePubMedPDF
- 9. Leigh RJ, Zee DS. The neurology of eye movements. 5th ed. Contemporary Neurology; 2015.
- 10. Lee SU. Vascular origin of central vertigo: brainstem. Res Vestib Sci 2021;20:1–6.ArticlePDF
- 11. Lee MY, Son HR, Rah YC, Jung JY, Suh MW. Recovery phase spontaneous nystagmus, its existence and clinical implication. J Audiol Otol 2019;23:33–8.ArticlePubMedPMCPDF
- 12. Kim JD. Neurophysiology of vestibular compensation. Audiol Speech Res 2023;19:1–16.ArticlePDF
- 13. Amarenco P, Hauw JJ. Cerebellar infarction in the territory of the anterior and inferior cerebellar artery. A clinicopathological study of 20 cases. Brain 1990;113(Pt 1):139–55.ArticlePubMed
- 14. A marenco P, Rosengart A, DeWitt LD, Pessin MS, Caplan LR. Anterior inferior cerebellar artery territory infarcts. Mechanisms and clinical features. Arch Neurol 1993;50:154–61.ArticlePubMed
- 15. Newman-Toker DE, Kerber KA, Hsieh YH, Pula JH, Omron R, Saber Tehrani AS, et al. HINTS outperforms ABCD2 to screen for stroke in acute continuous vertigo and dizziness. Acad Emerg Med 2013;20:986–96.PubMed
Citations
Citations to this article as recorded by




 PubReader
PubReader ePub Link
ePub Link Cite
Cite