Articles
- Page Path
- HOME > Res Vestib Sci > Volume 22(4); 2023 > Article
-
Case Report
자발 하향안진 및 보행장애를 동반한 아놀드-키아리 기형 -
김민범, 조윤진

- Arnold-Chiari Malformation Presented with Spontaneous Down-Beating Nystagmus and Gait Disturbance
-
Minbum Kim, Youn Jin Cho
-
Research in Vestibular Science 2023;22(4):132-136.
DOI: https://doi.org/10.21790/rvs.2023.22.4.132
Published online: December 15, 2023
Department of Otorhinolaryngology-Head & Neck Surgery, Catholic Kwandong University International St. Mary’s Hospital, Catholic Kwandong University College of Medicine, Incheon, Korea
- Corresponding Author: Minbum Kim Department of Otorhinolaryngology-Head & Neck Surgery, Catholic Kwandong University International St. Mary’s Hospital, 25 Simgok-ro 100beon-gil, Seo-gu, Incheon 22711, Korea Tel: +82-32-290-3052 Fax: +82-32-290-3050 E-mail: minbumkim78@gmail.com
Copyright © 2023 by The Korean Balance Society.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,169 Views
- 18 Download
Abstract
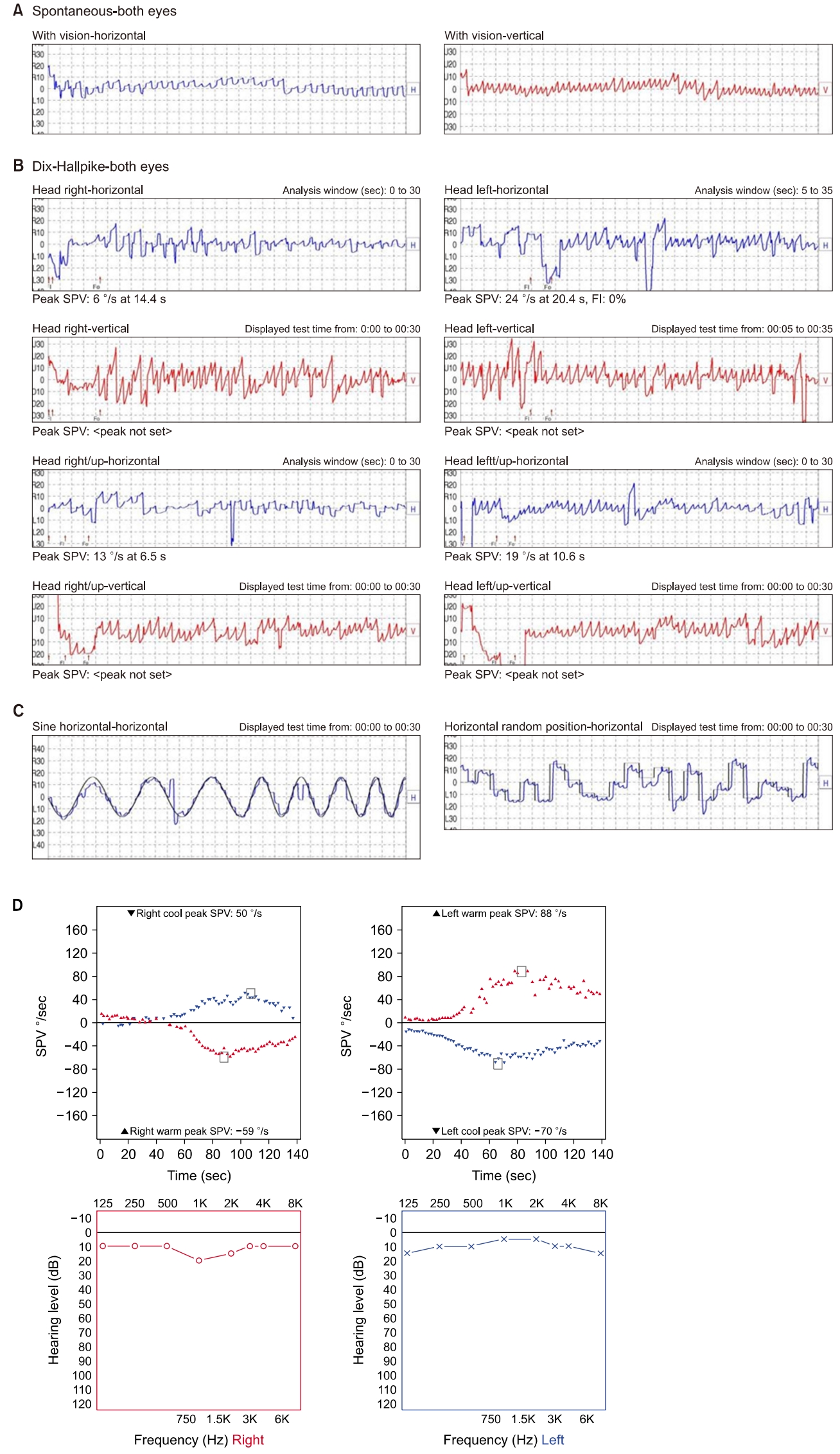
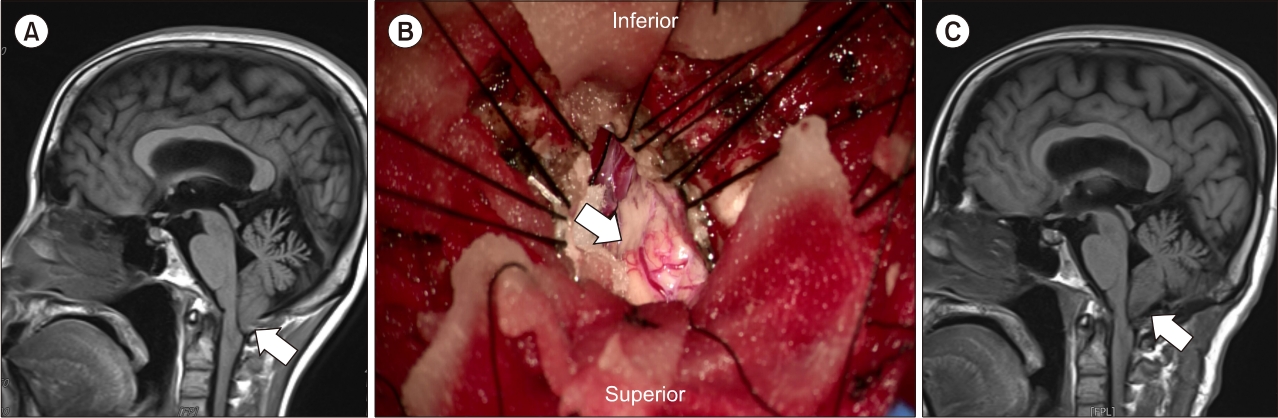
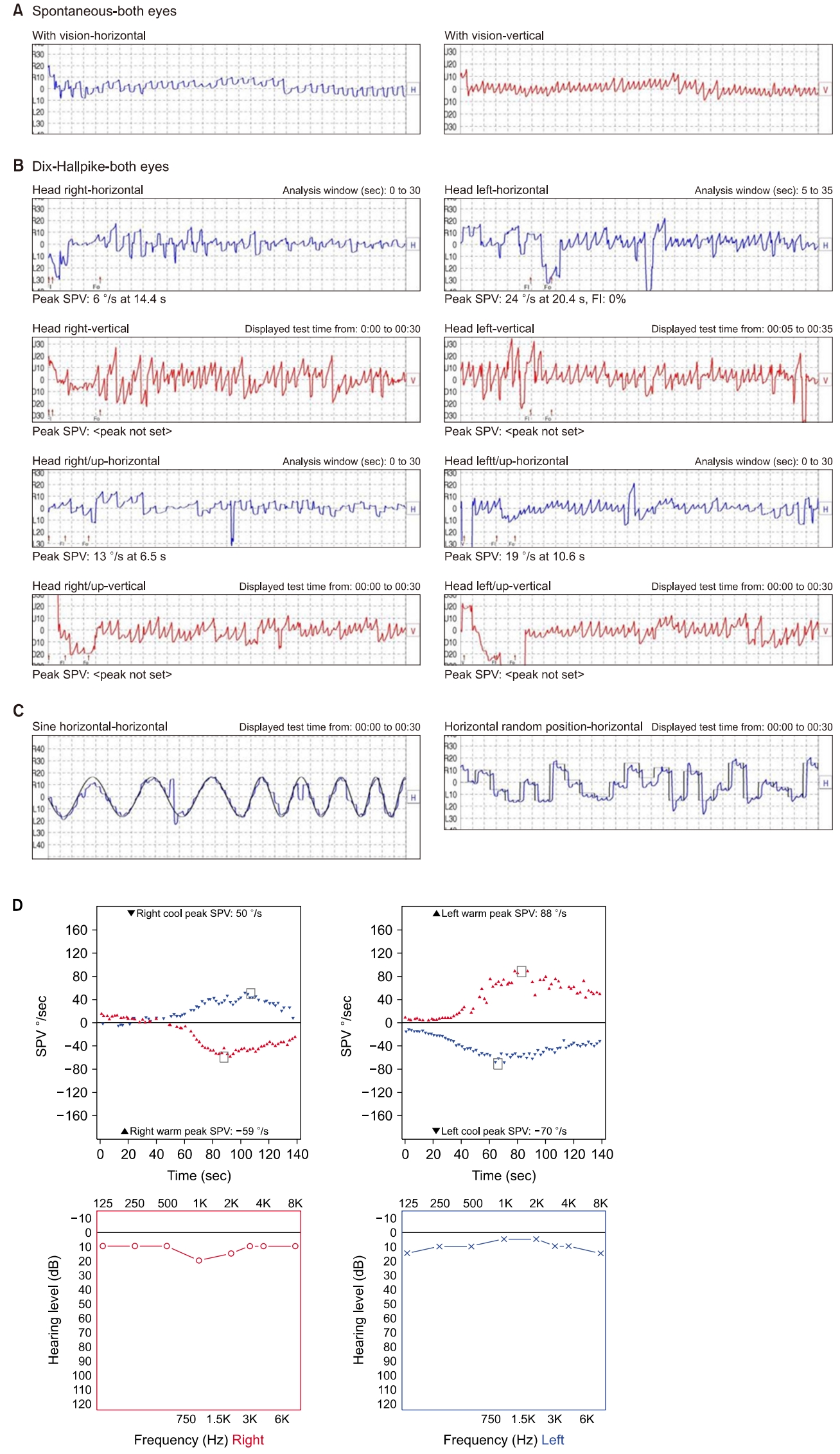
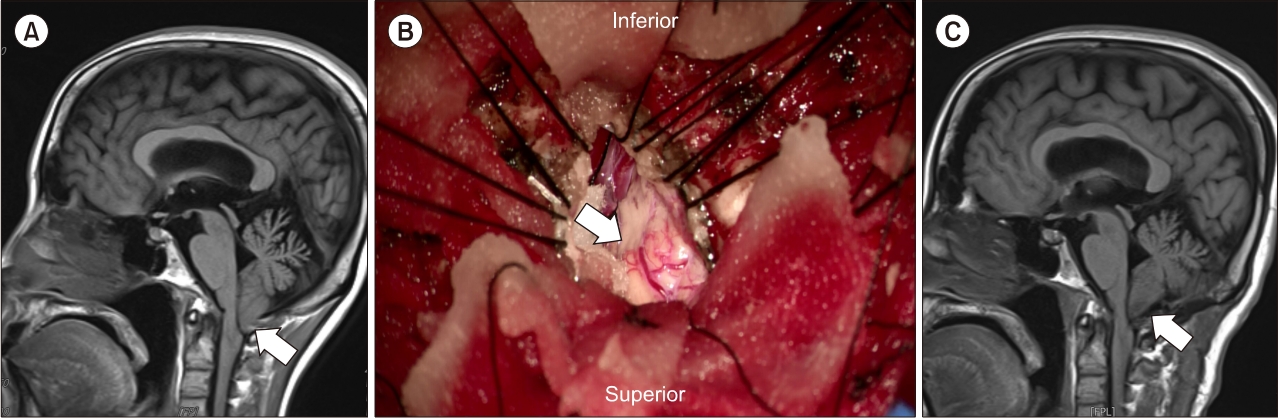
- Arnold Chiari malformation is a disease which is characterized by herniation of a portion of the cerebellum through the foramen magnum. Symptoms vary depending on the extent of the affected area, including posterior neck pain, upper limb pain, paralysis, paresthesia, weakness, dizziness, and ataxia. Among the patients presenting with dizziness, nystagmus is frequently observed, which is primarily characterized by down-beating nystagmus. We experienced a 42- years-old female patient presented with vertigo and gait disturbance, who were diagnosed with type 1 Arnold-Chiari malformation and treated by surgical decompression.
서 론
증 례
고 찰
-
이해관계(CONFLICT OF INTEREST)
저자들은 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.
-
연구 지원(FUNDING/SUPPORT)
이 연구는 2017년도 정부(교육과학기술부)의 재원으로 한국연구재단의 지원을 받아 수행된 기초연구사업입니다(NRF-2017R1D1A3B03030968).
-
저자 기여(AUTHOR CONTRIBUTIONS)
Conceptualization, Funding acquisition, Investigation, Visualization: MK; Data curation, Formal analysis, Methodology: MK, YJC; Writing–Original Draft: MK; Writing–Review & Editing: MK, YJC.
All authors read and approved the final manuscript.
ARTICLE INFORMATION
SUPPLEMENTARY MATERIALS
- 1. Russell GE, Wick B, Tang RA. Arnold-Chiari malformation. Optom Vis Sci 1992;69:242–7.ArticlePubMed
- 2. Kim KT, Jung I, Kim JS. Clinical characteristics of spontaneous downbeat nystagmus in Koreans: analysis of 218 cases. J Korean Neurol Assoc 2016;34:27–32.ArticlePDF
- 3. Wagner JN, Glaser M, Brandt T, Strupp M. Downbeat nystagmus: aetiology and comorbidity in 117 patients. J Neurol Neurosurg Psychiatry 2008;79:672–7.ArticlePubMed
- 4. Baloh RW, Spooner JW. Downbeat nystagmus: a type of central vestibular nystagmus. Neurology 1981;31:304–10.ArticlePubMed
- 5. Zee DS, Friendlich AR, Robinson DA. The mechanism of downbeat nystagmus. Arch Neurol 1974;30:227–37.ArticlePubMed
- 6. Halmagyi GM, Rudge P, Gresty MA, Sanders MD. ownbeating nystagmus. A review of 62 cases. Arch Neurol 1983;40:777–84.ArticlePubMed
- 7. Nakamagoe K, Iwamoto Y, Yoshida K. Evidence for brainstem structures participating in oculomotor integration. Science 2000;288:857–9.ArticlePubMed
- 8. Marti S, Straumann D, Glasauer S. The origin of downbeat nystagmus: an asymmetry in the distribution of on-directions of vertical gaze-velocity Purkinje cells. Ann N Y Acad Sci 2005;1039:548–53.ArticlePubMed
- 9. Böhmer A, Straumann D. Pathomechanism of mammalian downbeat nystagmus due to cerebellar lesion: a simple hypothesis. Neurosci Lett 1998;250:127–30.ArticlePubMed
- 10. Korres S, Balatsouras DG, Zournas C, Economou C, Gatsonis SD, Adamopoulos G. Periodic alternating nystagmus associated with Arnold-Chiari malformation. J Laryngol Otol 2001;115:1001–4.ArticlePubMed
- 11. Paul KS, Lye RH, Strang FA, Dutton J. Arnold-Chiari malformation. Review of 71 cases. J Neurosurg 1983;58:183–7.PubMed
- 12. Spooner JW, Baloh RW. Arnold-Chiari malformation: improvement in eye movements after surgical treatment. Brain 1981;104:51–60.ArticlePubMed
- 13. Mossman SS, Bronstein AM, Gresty MA, Kendall B, Rudge P. Convergence nystagmus associated with Arnold-Chiari malformation. Arch Neurol 1990;47:357–9.ArticlePubMed
- 14. Nakahara H, Murofushi T. Congenital-type nystagmus in Arnold-Chiari malformation. Otolaryngol Head Neck Surg 2003;128:598–600.ArticlePubMedPDF
- 15. Ghasia FF, Gulati D, Westbrook EL, Shaikh AG. Viewing condition dependence of the gaze-evoked nystagmus in Arnold Chiari type 1 malformation. J Neurol Sci 2014;339:134–9.ArticlePubMed
- 16. Kumar A, Pieri A, Krol G. Rebound caloric nystagmus. Laryngoscope 1993;103:1205–13.ArticlePubMed
- 17. Pedersen RA, Troost BT, Abel LA, Zorub D. Intermittent downbeat nystagmus and oscillopsia reversed by suboccipital craniectomy. Neurology 1980;30:1239–42.ArticlePubMed
- 18. Strahle J, Muraszko KM, Kapurch J, Bapuraj JR, Garton HJ, Maher CO. Natural history of Chiari malformation Type I following decision for conservative treatment. J Neurosurg Pediatr 2011;8:214–21.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite