Abstract
- Intracranial dural arteriovenous fistula (dAVF) is characterized by an abnormal connection between branches of arteries and veins in the dura mater. Clinical manifestations of dAVF vary depending on their location, feeder arterial supply, amount of shunting, and most importantly, their venous drainage pattern. Acute vertigo has been rarely reported as an initial presentation of dAVF due to venous congestion in the brainstem. We report a patient who presented with acute right vestibulopathy without any brainstem signs in dAVF involving the transversesigmoid sinus. The patient showed abnormal caloric response but normal head impulse in the affected ear. Without any treatment, the patient’s symptoms gradually improved with a normalization of right canal paresis. Follow-up cerebral angiography also revealed a spontaneous regression of the shunt flow and reduction of venous drainage at the right transverse-sigmoid sinus. Based on the results of vestibular function tests and cerebral angiography, acute vertigo in our patient may be ascribed to impaired reabsorption of endolymph by focal venous congestion.
-
Keywords: Dural arteriovenous fistula; Vertigo; Caloric paresis
-
중심단어: 경막동정맥루, 현훈, 반고리관마비
INTRODUCTION
Intracranial dural arteriovenous fistula (dAVF) is an unusual cerebral vascular malformation characterized by an abnormal connection between branches of arteries and veins in the dura mater [1]. A dAVF can present with a myriad of clinical symptoms and signs. In general, the location and venous drainage pattern are important factors that determine their clinical presentation and potential for serious sequelae [1]. Generalized central nervous system symptoms including headache, seizure, and focal neurological deficits may result from the cortical venous drainage, while dAVF involving particular areas of the brain may cause less aggressive symptoms such as pulsatile tinnitus and orbital symptoms. Rarely, acute vertigo has been also reported as an initial presentation of dAVF due to venous congestion in the brainstem [2-6]. We report a patient who presented with acute right vestibulopathy without any brainstem signs in dAVF involving the transverse-sigmoid sinus.
This study followed the tenets of the Declaration of Helsinki, and was approved by the Institutional Review Board of Pusan National University Yangsan Hospital (No. 55-2023-053).
CASE REPORT
A 62-year-old female patient developed acute spontaneous vertigo with vomiting and unsteadiness. She had tinnitus in the left ear 2 months ago. Examination 3 days after vertigo onset showed spontaneous left-beating horizontal-torsional nystagmus that increased during left eccentric gaze and with removal of visual fixation. Other neurological examinations were unremarkable. Bedside head impulse tests were normal, which was quantitatively documented by video-based equipment (SLMED) (Fig. 1A). However, bithermal caloric irrigation showed a canal paresis (CP) in the right side (42%) (Fig. 1B). The subjective visual vertical (SVV) was tilted toward the right side (left eye, 7.4°; right eye, 5.8°; binocular measurements, 4.5°; normal ranges, ‒3.0° to 3.0°; positive value indicates rightward tilt). Pure tone audiometry exhibited conductive hearing loss in the left ear. Brain magnetic resonance imaging (MRI) with diffusion-weighted images detected no abnormal high signal intensity, but magnetic resonance angiography revealed a vascular abnormality suggestive of dAVF in the right skull base (Fig. 2A, B). Digital subtraction cerebral angiography (DSA) confirmed dAVF at the right transverse-sigmoid junction with multiple arterial feeders including the right ascending pharyngeal artery and both middle meningeal arteries (Fig. 2D). The fistula drainage was mainly antegrade flow into the right sigmoid and internal jugular veins, but there was also retrograde drainage into the left transverse sinus. Due to increased pressure of the right transverse-sigmoid sinus, normal cerebral drainage was also performed via the left transverse-sigmoid sinus. Because dAVF was too diffuse and of immature type, and it was difficult to identify the angiographic anatomy of the feeders, endovascular treatment was not performed. The patient was discharged with mild dizziness and unsteadiness 10 days after symptom onset.
At the 3-month follow-up, the patient had no dizziness and unsteadiness but still complained of the left tinnitus. There was no spontaneous nystagmus with and without fixation, and bithermal caloric tests were normalized. Follow-up DSA revealed that the amount of shunt flow was markedly decreased with the reduction of the feeder’s diameter compared to the results of the initial DSA (Fig. 3A). During a 2-year follow-up period, the patient remained symptom-free despite the persistence of the left tinnitus. Because dAVF was changed into a restrictive phase with the spontaneous regression of the shunt flow at the latest follow-up DSA, further treatment was not performed (Fig. 3B).
DISCUSSION
Our patient developed acute right vestibulopathy as an initial presentation of dAVF. To the best of our knowledge, this is the first documentation of vestibular dysfunction in a patient with vertigo caused by dAVF.
Clinical manifestations of dAVF depend on their location, feeder arterial supply, amount of shunting, and most importantly, their venous drainage pattern [1]. Cortical venous drainage may lead to more aggressive clinical presentations including sudden onset of severe headache, seizures, focal neurological deficits, and intracranial hemorrhage. On the other hand, increased dural sinus blood flow in particular areas of the brain may cause less aggressive symptoms such as pulsatile tinnitus in dAVF involving the transverse and sigmoid sinus. Dizziness or vertigo can also be observed in patients with dAVF due to edematous or ischemic change in the brainstem [2-6]. Most patients with dizziness/vertigo showed venous congestion with edema in the brainstem on brain MRI and had other coexisting brainstem signs such as motor weakness, bulbar palsy, or Horner syndrome.
By contrast, our patient had isolated vertigo without other neurological signs and the edematous or ischemic change in the brainstem. Instead, vestibular function tests showed a spontaneous left-beating nystagmus with the right CP and SVV tilt, suggesting a right peripheral vestibulopathy. The venous blood from most of the vestibular apparatus is drained into the sigmoid sinus via the vein of the vestibular aqueduct (VVA) [7]. The VVA courses near the endolymphatic sac, operculum, and sigmoid sinus and is potentially vulnerable to expanding structures in the cranial posterior fossa [8]. In our patient, cerebral angiography revealed a dAVF at the right transverse-sigmoid junction, which drained into the right internal jugular vein through the transverse and sigmoid sinus. Thus, the fistula may cause focal venous congestion around the right transverse-sigmoid junction, resulting in increased fluid pressure in the right inner ear and subsequently leading to vestibular dysfunction. Experimental studies demonstrated pathological changes in the vestibular apparatus by venous obstruction of the labyrinth [7]. Likewise, cerebral venous thrombosis involving the transverse and sigmoid sinus has been reported in a patient with acute peripheral vestibulopathy or sudden sensorineural hearing loss [9,10].
Alternatively, the endolymphatic hydrops in the vestibular apparatus may lead to acute vertigo. Our patient showed normal head impulses despite the right CP. This dissociation between the two tests has been commonly reported in Menière’s disease, which is considered a consequence of the hydropic expansion of the semicircular duct [11,12]. The enlarged diameter of the duct may generate a local convective flow, thus dissipating the hydrostatic force across the cupula, so the response to caloric stimulation will be diminished. However, this expansion does not significantly affect the response of the angular acceleration stimulation with high speed, resulting in normal head impulses. Thus, abnormal caloric response with normal head impulse may be associated with endolymphatic hydrops in the inner ear [12]. In our patient, there was focal congestion and dilation of the right sigmoid and internal jugular veins due to antegrade drainage of the fistula. This may put pressure on the endolymphatic sac and duct, resulting in an impaired reabsorption of endolymph and endolymphatic hydrops, as can be seen in high jugular bulb [13]. Moreover, when the venous drainage decreased with the reduction of shunt flow at follow-up angiography, bithermal caloric tests showed the resolution of the right CP. Previous studies have also described Menière’s disease-like symptoms caused by impeded drainage of the VVA [14,15]. To identify the association between vestibular dysfunction and dAVF involving the transverse-sigmoid sinus, further study using the inner ear MRI may be needed.
Interestingly, the shunt flow in our patient gradually decreased without any treatment. As the amount of shunt flow decreases, the patient’s symptoms also improved with the normalization of the right CP. The natural history of dAVFs is somewhat uncertain, but spontaneous regression has been rarely reported [16]. This particular evolution may result from the thrombosis of the feeder arteries, the mass effect related to hematoma, or vasospasm [16].
ARTICLE INFORMATION
-
CONFLICT OF INTEREST
저자 중 오은혜는 Research in Vestibular Science의 편집간사이며, 본 논문의 심사과정에 관여하지 않았습니다. 그 외 저자들은 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.
-
FUNDING/SUPPORT
This study was supported by a 2023 research grant from Pusan National University Yangsan Hospital.
-
AUTHOUR CONTRIBUTIONS
Conceptualization: All authors; Data curation: WJS, JR; Investigation: EHO; Funding acquisition, Supervision: JHC; Writing-Original: WJS; Writing-Review & Editing: All authors.
All authors read and approved the final manuscript.
Fig. 1.(A) The findings of video head impulse tests are normal for all six semicircular canals. Normal gain for the horizontal canals (HCs) is 0.89–1.02, for the posterior canals (PCs) is 0.88–1.09, and for the anterior canals (ACs) is 0.80–1.18. (B) Bithermal caloric tests show the right canal paresis (42%).

Fig. 2.(A) Diffusion-weighted magnetic resonance imaging shows no acute lesion in the pons. (B) Magnetic resonance angiography discloses abnormal signal intensity in the right skull base, indicating venous drainage. (C, D) Digital subtraction cerebral angiography of the right external carotid artery demonstrates a dural arteriovenous fistula (dAVF) fed by the ascending pharyngeal and middle meningeal arteries. The dAVF mainly drains into the internal jugular vein via sigmoid sinus, but retrograde drainage via the transverse sinus is also observed.

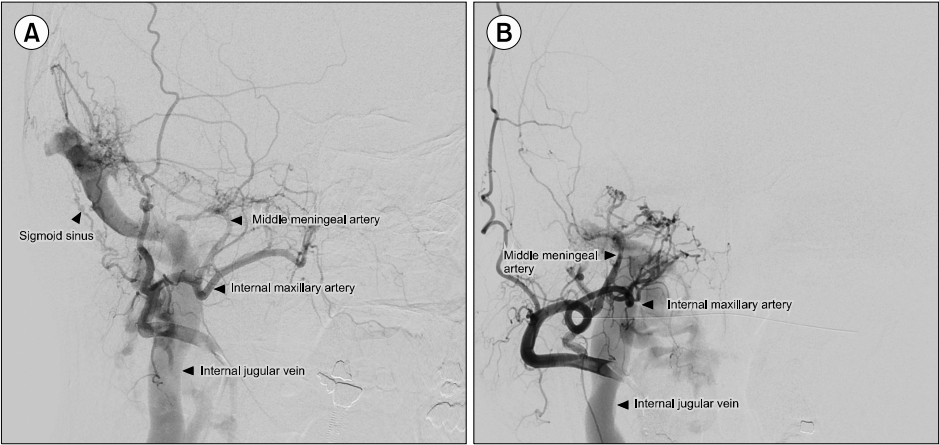
Fig. 3.(A) At the 3-month followup angiography, the amount of shunt flow is decreased with the reduction of the feeder’s diameter compared to the initial angiography and retrograde drainage via the transverse sinus is not observed. (B) The 2-year follow-up angiography shows that dAVF is changed into a restrictive phase with the regression of the shunt flow.

REFERENCES
- 1. Miller TR, Gandhi D. Intracranial dural arteriovenous fistulae: clinical presentation and management strategies. Stroke 2015;46:2017–25.ArticlePubMed
- 2. Chen PY, Juan YH, Lin SK. An isolated unilateral pontomedullary lesion due to an intracranial dural arteriovenous fistula mimicking a brain tumor: case and review. J Nippon Med Sch 2019;86:48–54.ArticlePubMed
- 3. Wigansari GP, Sani AF, Kurniawan D, Qimindra FR. Chronic pulsatile tinnitus and continuous vertigo due to very delayed diagnosis of single slow-flow dural arteriovenous. J Neurosci Rural Pract 2023;14:140–2.ArticlePubMedPMC
- 4. Shimizu A, Ishikawa T, Yamaguchi K, Funatsu T, Ryu B, Nagahara A, et al. Brainstem venous congestion caused by perimedullary drainage in anterior cranial fossa dural arteriovenous fistula. World Neurosurg 2019;127:503–8.ArticlePubMed
- 5. Satoh M, Kuriyama M, Fujiwara T, Tokunaga K, Sugiu K. Brain stem ischemia from intracranial dural arteriovenous fistula: case report. Surg Neurol 2005;64:341–5.ArticlePubMed
- 6. Takahashi S, Tomura N, Watarai J, Mizoi K, Manabe H. Dural arteriovenous fistula of the cavernous sinus with venous congestion of the brain stem: report of two cases. AJNR Am J Neuroradiol 1999;20:886–8.PubMedPMC
- 7. Griffith AN. Venous obstruction of the labyrinth: some experimental and anatomical studies. Proc R Soc Med 1961;54:917–22.ArticlePubMedPMCPDF
- 8. Friis M, Sørensen MS, Qvortrup K. The vein of the vestibular aqueduct with potential pathologic perspectives. Otol Neurotol 2008;29:73–8.ArticlePubMed
- 9. Kim HA, Lee H, Park BR. Unilateral peripheral vestibulopathy associated with cerebral venous infarction. J Korean Bal Soc 2006;5:285–7.
- 10. Kang TH, Jang JY, Cho KY, Joo JK, Lee TH, Sung SM, et al. Cerebral venous sinus thrombosis developed during infertility treatment in a male patient. J Korean Neurol Assoc 2015;33:358–60.ArticlePDF
- 11. Kim HS, Oh EH, Kim JY, Choi SY, Choi KD, Choi JH. Discordant vestibulo-ocular reflex function according to the frequency and mode of stimulation. J Neurol 2022;269:4742–52.ArticlePubMedPDF
- 12. McGarvie LA, Curthoys IS, MacDougall HG, Halmagyi GM. What does the head impulse test versus caloric dissociation reveal about vestibular dysfunction in Ménière's disease? Ann N Y Acad Sci 2015;1343:58–62.ArticlePubMed
- 13. Hu J, Peng A, Deng K, Huang C, Wang Q, Pan X, et al. Value of CT and three-dimensional reconstruction revealing specific radiological signs for screening causative high jugular bulb in patients with Meniere's disease. BMC Med Imaging 2020;20:103. ArticlePubMedPMCPDF
- 14. Scaramella JG. Hyperhomocysteinemia and left internal jugular vein thrombosis with Ménière's symptom complex. Ear Nose Throat J 2003;82:856–65.ArticlePubMedPDF
- 15. Couloigner V, Grayeli AB, Bouccara D, Julien N, Sterkers O. Surgical treatment of the high jugular bulb in patients with Ménière's disease and pulsatile tinnitus. Eur Arch Otorhinolaryngol 1999;256:224–9.ArticlePubMedPDF
- 16. Clarençon F, Biondi A, Sourou NA, Di Maria F, Iosif C, Nouet A, et al. Spontaneous closure of intracranial dural arteriovenous fistulas: a report of 3 cases. Clin Neurol Neurosurg 2013;115:971–5.ArticlePubMed
Citations
Citations to this article as recorded by




 PubReader
PubReader ePub Link
ePub Link Cite
Cite