Abstract
- A 61-year-old male patient undergoing chemotherapy for esophageal cancer presented with symptoms of rightward tilting while both sitting and walking. A neurological examination revealed a head tilt, skew deviation with hypertrophy of the left eye, and a rightward shift in his gait. No spontaneous nystagmus was observed, and the vestibulo-ocular reflex was normal. Magnetic resonance imaging of the head revealed a suspected metastatic lesion in the right medial prefrontal cortex. Following the initiation of levetiracetam treatment, the patient demonstrated marked improvement, with the resolution of both head tilt and skew deviation within 1 month. Traditionally, the ocular tilt reaction has been attributed to unilateral or asymmetric dysfunction of the graviceptive pathways extending from the utricle to the upper midbrain lesions. However, this case highlights the potential involvement of the prefrontal cortex in the ocular tilt reaction. Further research is warranted on the role of the prefrontal cortex within the vestibular system.
-
Keywords: Vestibular system; Frontal lobe; Skew deviation
INTRODUCTION
Clinical signs of vestibular tone imbalance in the roll plane include complete ocular tilt or its components, such as head tilt, ocular torsion, skew deviation, and subjective visual vertical tilt [1]. Ocular tilt and its components arise from an imbalance in the vestibulo-ocular reflex due to unilateral peripheral vestibular damage or unilateral lesions of the central vestibular pathways in the brainstem [2]. Lesions in the brainstem caudal to the medulla oblongata, which affect the vestibular nerve and vestibular nucleus, cause ipsilateral head tilt. In contrast, lesions at the level of the midbrain, impacting the medial longitudinal fasciculus and the interstitial nucleus of Cajal, result in contralateral head tilt [3,4]. It is recognized that lesions in the vestibular thalamus or vestibular cortex, such as the posterior insula, may lead to vestibular dysfunction manifesting as perceptual visual vertical tilt. However, there have been no documented cases of complete ocular tilt accompanied by subjective visual vertical tilt in cortical lesions. Here, the authors present a case of complete ocular tilt with subjective visual vertical tilt in a patient with a lesion in the medial prefrontal cortex.
CASE REPORT
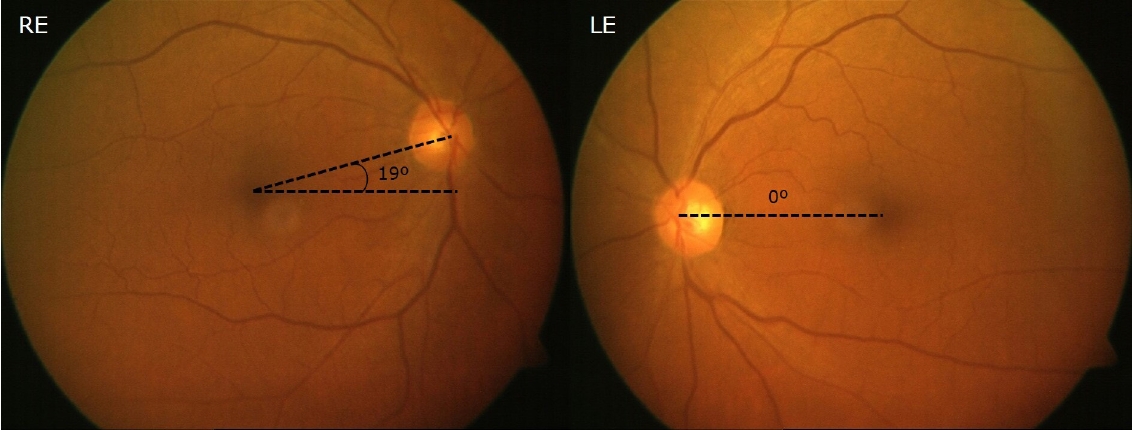
A 61-year-old man, who was undergoing his fourth cycle of 5-fluorouracil/cisplatin followed by four cycles of docetaxel/cisplatin as neoadjuvant chemotherapy for esophageal cancer, was referred to the neurology department due to experiencing a rightward tilt while sitting. The patient also exhibited a slight rightward tilt when walking. Neurological examination revealed a head tilt, skew deviation with hypertrophy of the left eye, and a rightward shift in his gait. However, no abnormalities were found in other tests, including those assessing brainstem and cerebellar function. Video-oculography did not reveal spontaneous nystagmus, gaze-evoked nystagmus, or head-shaking nystagmus. Bilateral saccadic gains were diminished, but there was no over- or under-shooting of saccades. Additionally, pursuit eye movements were reduced on both sides, and cogwheel pursuit eye movements were noted. The vestibulo-ocular reflex was normal as assessed by the caloric test and the head thrust test. The subjective visual axis was tilted 5.4° to the right, and a 19° rightward ocular torsion was observed (Fig. 1). Ocular and cervical vestibular evoked myogenic potentials were within normal limits.
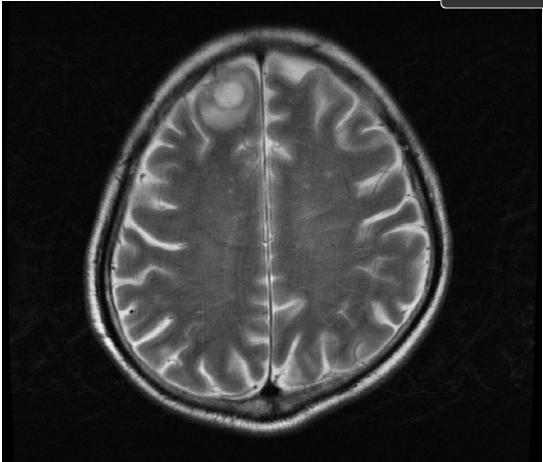
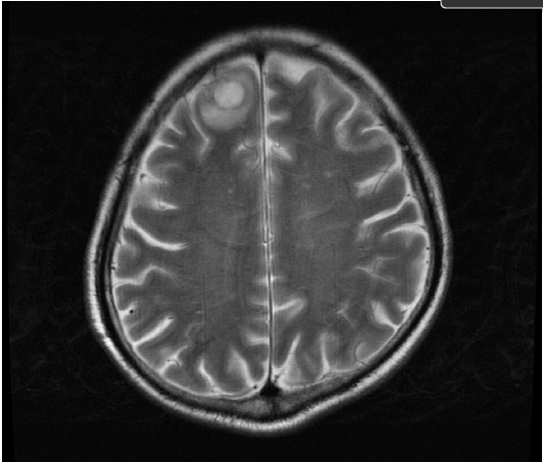
Magnetic resonance imaging (MRI) of the head revealed a suspected metastatic lesion in the right medial prefrontal cortex (Fig. 2). An electroencephalogram demonstrated sharp waves predominantly in the right frontal cortex. Given the probability of a partial seizure, the patient was administered 500 mg of levetiracetam and underwent one course of palliative radiotherapy targeting the metastatic lesion. The patient exhibited a gradual improvement in symptoms; the head tilt and skew deviation were no longer present after one month of follow-up. Saccades and pursuit eye movements appeared normal upon video-oculography. Although no further treatment was administered, the symptoms of tilting did not recur while the patient continued on anticonvulsant therapy.
This study was approved by the Institutional Review Board of Keimyung University School of Medicine (No. 2023-11-032). Written informed consent was obtained for publication of this case report and accompanying images.
DISCUSSION
Ocular tilt and its components result from an imbalance in the vestibulo-ocular reflex due to either unilateral peripheral vestibular damage or unilateral lesions in the central vestibular pathways within the brainstem [2,5]. Although lesions in the vestibular thalamus or vestibular cortex, such as the posterior insula, are not known to cause an ocular tilt reaction, they may induce a subjective visual vertical tilt [6]. To date, there have been no studies investigating the ocular tilt reaction, as opposed to subjective visual vertical tilt, in the context of nonvestibular cortical lesions.
Previous studies have found that the prefrontal cortex is involved in eye movements and visuospatial orientation. A case report on epileptic vertigo described a patient who experienced rotational vertigo without nystagmus. This condition was linked to interictal spikes originating in the left frontal lobe. The authors suggested that the vertigo was due to ictal discharges emanating from regions within the prefrontal cortex that represent vestibular functions [7]. Although the cortical representations of the vestibular system are typically located in the parietal and temporal lobes in humans, a study using positron emission tomography for vestibular activation also indicated frontal lobe involvement [8]. Furthermore, a functional MRI study that measured changes in the blood-oxygenation-level-dependent signal during vestibular galvanic (mastoid) stimulation provided evidence of multisensory integration processes in the cortex including the prefrontal cortical areas during vestibular stimulation [9].
It is widely recognized that the ocular tilt reaction is induced by stimulation of the semicircular canal and the otolith organs, especially the utricle. However, there is a lack of research on the cerebral cortical response to utricular stimulation. Furthermore, various studies investigating cerebral cortical responses during the cervical vestibular evoked myogenic potentials test have reported activity in multiple cerebral areas, including the prefrontal cortex [10,11]. There is a need for future research to explore the ocular tilt reaction in relation to damage to the frontal lobe, specifically the prefrontal cortex.
Since the patient in the current case showed improvement following the administration of levetiracetam, it is possible that the ocular tilt reaction was caused by an irritative lesion. In cases of cortical lesions, the subjective visual vertical typically tilts toward the side opposite the lesion. This is believed to result from the involvement of the parietoinsular vestibular cortex or the superior temporal gyrus, both of which are components of the vestibular cortex. Although there was no direct involvement of the vestibular cortex in this case, the rightward tilt of the subjective visual vertical, induced by the irritative lesion on the right side, aligns with findings reported in the literature.
The ototoxicity of docetaxel is well-recognized; however, it typically manifests early in the course of chemotherapy [12]. In this case, an association with peripheral vestibular dysfunction is highly unlikely, because the patient completed four cycles of chemotherapy and did not have any abnormal findings on the vestibular function test.
ARTICLE INFORMATION
-
Funding/Support
None.
-
Conflicts of Interest
Hyung Lee is an editor of Research in Vestibular Science, Frontiers in Neuro-otology, and Current Medical Imaging Review. The authors declare that they have no conflicts of interest related to this article.
-
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article. For other data, these may be requested through the corresponding author.
-
Authors's Contributions
Conceptualization, Investigation, Methodology, Data curation, Formal analysis, Project administration, Visualization: HAK; Formal analysis, Project administration: HL; Writing–original draft: HAK; Writing–review & editing: HL.
All authors read and approved the final manuscript.
Fig. 1.Ocular fundoscopy shows extorsion on the right eye (RE) and intorsion on the left eye (LE).
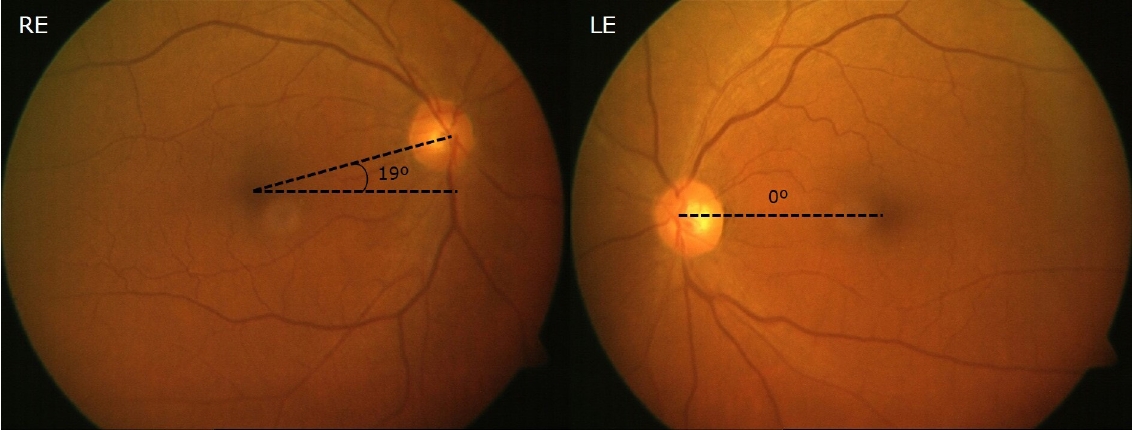
Fig. 2.Brain magnetic resonance imaging of the patient shows a metastatic lesion in the right medial prefrontal cortex.
REFERENCES
- 1. Westheimer G, Blair SM. The ocular tilt reaction--a brainstem oculomotor routine. Invest Ophthalmol 1975;14:833–839.PubMed
- 2. Halmagyi GM, Gresty MA, Gibson WP. Ocular tilt reaction with peripheral vestibular lesion. Ann Neurol 1979;6:80–83.ArticlePubMed
- 3. Brandt T, Dieterich M. Skew deviation with ocular torsion: a vestibular brainstem sign of topographic diagnostic value. Ann Neurol 1993;33:528–534.ArticlePubMed
- 4. Halmagyi GM, Brandt T, Dieterich M, Curthoys IS, Stark RJ, Hoyt WF. Tonic contraversive ocular tilt reaction due to unilateral meso-diencephalic lesion. Neurology 1990;40:1503–1509.ArticlePubMed
- 5. Dieterich M, Brandt T. The bilateral central vestibular system: its pathways, functions, and disorders. Ann N Y Acad Sci 2015;1343:10–26.ArticlePubMed
- 6. Baier B, Suchan J, Karnath HO, Dieterich M. Neural correlates of disturbed perception of verticality. Neurology 2012;78:728–735.ArticlePubMed
- 7. Kluge M, Beyenburg S, Fernández G, Elger CE. Epileptic vertigo: evidence for vestibular representation in human frontal cortex. Neurology 2000;55:1906–1908.ArticlePubMed
- 8. Bottini G, Sterzi R, Paulesu E, et al. Identification of the central vestibular projections in man: a positron emission tomography activation study. Exp Brain Res 1994;99:164–169.ArticlePubMedPDF
- 9. Bense S, Stephan T, Yousry TA, Brandt T, Dieterich M. Multisensory cortical signal increases and decreases during vestibular galvanic stimulation (fMRI). J Neurophysiol 2001;85:886–899.ArticlePubMed
- 10. Ertl M, Moser M, Boegle R, Conrad J, Zu Eulenburg P, Dieterich M. The cortical spatiotemporal correlate of otolith stimulation: vestibular evoked potentials by body translations. Neuroimage 2017;155:50–59.ArticlePubMed
- 11. Schlindwein P, Mueller M, Bauermann T, Brandt T, Stoeter P, Dieterich M. Cortical representation of saccular vestibular stimulation: VEMPs in fMRI. Neuroimage 2008;39:19–31.ArticlePubMed
- 12. Sarafraz M, Ahmadi K. Paraclinical evaluation of side-effects of Taxanes on auditory system. Acta Otorhinolaryngol Ital 2008;28:239–242.PubMedPMC
Citations
Citations to this article as recorded by


 , Hyun Ah Kim
, Hyun Ah Kim
 PubReader
PubReader ePub Link
ePub Link Cite
Cite